I will tell you my point of vue on this question :
Marc has a lot of friends
But honestly I did maximum in order to get all children’s and parents « on my sight « after Marc accsident at the beginning it was not obvious …
It’s exactly what I am doing :
Social life is very very important target so during 2 years II worked for this goal for Marc
I see results this year …( I have a chance because I am « not working mum » but in fact I do my job exactly this way : who can invite 5-6 neurological normal friends at home every week and play with them during 3-4 hours per day????….. so I am not working mum who do it for my child… i think I invest better than any proffecionel in this point….)
But I need professionals in parts I can’t do… 😉
Others parents don’t want to do efforts for your child ( or at least not much who will do)
It’s like this
It’s reality
When you know this and do all yourself without counting on them everything is easygoing…
And if it’s interesting to come to your home to theirs children’s they will ask to come from their parents and so … you will start invite for weekend for cake and coffee …. so you start create sosial links with parents and children’s….
Just don’t wait that they will invite you in reteurn
It’s will be always you who will do much more than others parents 😉
Yes it’s the best motivation for my son Marc so that’s why I do my own “friends” programm and every week planing ( yes you need to send messages /phone calls in order to plan 5-6 invitations per week).
Often parents they don’t have time / motivation to play with theirs children’s at home ( I do have this time and my hasbend is playing with kids just exeptional during weekends ! They love to play with him)
I know 11 children’s from his class and parents and we continue doing new friends of cause absolutely!
(so well I know to play with them in social games somtimes can be very boring for adults and we as parents somtimes wants just to rest I know all this! ) I have à chance naw Marc can a bit play just alone between children’s but it wasn’t so evident 2 years ago …
and yes somtimes I am inviting 2 his best friends ( boys) to sleep at home so we can have pyjamas parties 😉 and dansing 😉
Yes I will tell you it’s a lot of job /coking/playing
But it’s worth 😉
But you can’t imagine what I feel this year when children’s I don’t know yet from his class comme to me and ask : “ please can you invite me to eat with Marc?” I am also in his clas I am his friend”… and so – I ask marc” hey you know this boy you want invite him home?”
And his pleasure to tel me yes I want yes he is playing with me at school ….or So other day “mum can you invite this boy …etc…”
This is really cool feeling….
A lot of job but so cool!
🙂
It is a long way but it’s worth !
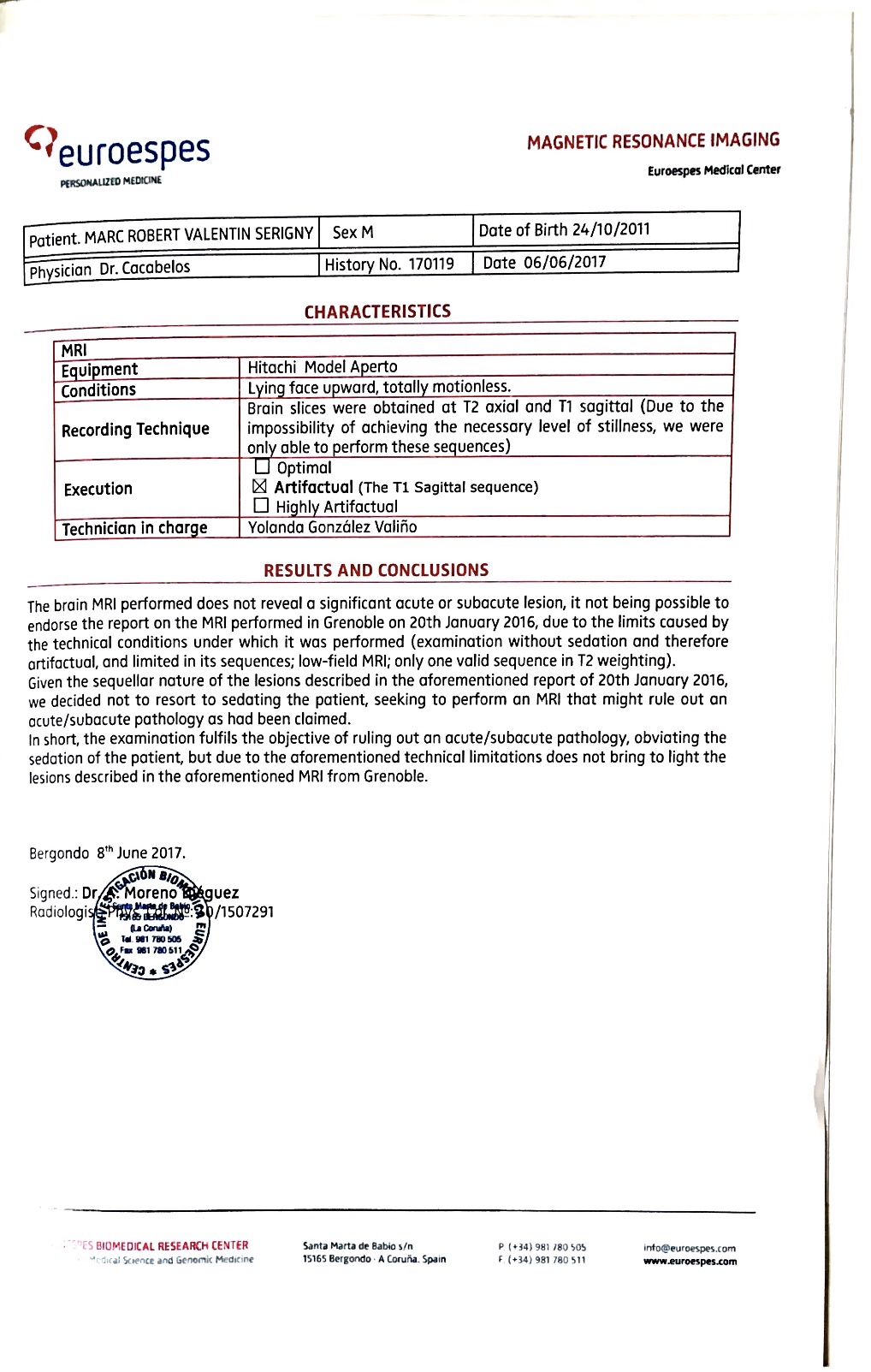
AS said it took me 2 years to get back Marc socialisation after his Sudden Cardiac Arrest.
I started with 2 best friends invited regulary at home ( for 2-3 hours) – weekend.
Than I started to invite friends to eat with Marc at home during lunches ( it’s of cause me who organize all I am going to school taking children’s / make them eat together and playing – and bring them back to school) – parents need only tell to school that they give me permission to take their children’s for lunch ( so not much trouble for other parents or any trouble for their daily plans)
Naw I am in fact : at level 3 lunches per week ( every time I invite only one friend )
And Friday evening – very often he is playing with friends ( after school)
And 2 others children’s for 4 hours invited to play each Saturday and Sunday !
Yah planing for Ministry of Foreign Affaires has less appointments 😉
( exept week-end we travel of cause)
So 6 friends per week!
It’s a real job I have 😉
Kids club
But it’s so worth it!
And if you know haw Marc is happy to has all his friends !
Et maintenant en français : ( désolé mon français n’est pas parfait … mais ça m’empêche pas ni parler ni écrire 😉
Je vais vous dire mon point de vue sur cette question: Marc a beaucoup d’amis!
Mais honnêtement j’ai fait le maximum pour avoir tous les enfants et parents «à ma vue» après l’accident de Marc au début ce n’était pas évident …
C’est mon travail de maman de lui aider pour acceptation sociale, je compte pas sur Ecole où metresse pour ça ( ils ont assez de travail déjà…) mais même pour les enfants « nerotypic » c’est aussi pas tout les enfants qui sont accepter donc pourquoi ? …. je me souviens quand j’étais petite un garçon ( ordinaire) en classe été très » populaire » …. son père investis beaucoup a l’école – organiser et participer dans sortie de l’école et des jeux » organisés de l’école » tout les enfants de l’école connaissait lui c’esta père de Valera et ce garçon en faite – était tes populaire par ce que son père a aider de devenir comme ça….. donc j’ai beaucoup réfléchis….
C’est exactement ce que je fais: la vie sociale est une cible très très importante donc pendant 2 ans j’ai travaillé pour cet objectif pour Marc.
Je vois des résultats cette année …2019-2020
(J’ai une chance car je ne «travaille pas» mais en fait je le fais mon travail exactement de cette façon: qui peut inviter 5-6 amis neurologiques normaux à la maison chaque semaine et jouer avec eux pendant 3-4 heures par jour ???? ….. donc je ne travaille pas officiellement – je suis une maman qui » travaille » que pour mon fils qui le ferait pour moi enfant … sauf moi???? Personne…. est que on peut réussir faire ça en restant maman qui travail – et lesse école gérer vie sociale de leur enfant ? Je ne sais pas….
je pense que j’investis mieux que n’importe quel proffecionel dans ce point peut faire. Mais j’ai besoin de professionnels dans des parties que je ne peux pas faire …( pas pour son vie sociale pour reheducations biensure) 😉
Les autres parents ne veulent pas faire des efforts pour votre enfant – surtout si il a un handicap – ils ont aussi PEUR de prendre quelconque responsabilité pour votre enfant – et c’est normal – ils ont peur…..(ou à du moins pas beaucoup qui fera inviter votre enfant en retour)….. si vous l’accompagner – pour les anniversaires – oui biensure ils inviteront !!!!
C’est comme ça
C’est la réalité
Quand vous savez cela et faites tout vous-même sans compter sur eux tout devient claire et facile…
Et s’il est intéressant de venir chez vous pour les enfants, ils demanderont à leurs parents de venir ( fait en sorte que vôtre maison devienne très intéressant pour eux à venir – un endroit où ils s’amuse vraiment super bien – camp de vacances ! ) et donc … vous commencerez à inviter le week-end pour un gâteau et un café …. alors vous commencerez à créer des liens sosiaux avec parents et enfants …. N’attendez pas qu’ils vous invitent en retour – quelque parents feront mais c’est vraiment pas important que vous le feraient 10 fois plus – par se que en fin compte c’est vôtre enfant qui sera gagnant.
Ca sera toujours vous qui ferez bien plus que les autres parents ( eux ils travail ! Et eux ils ont pas » besoin » de faire un effort supliment aire pour vie sociale de leur progéniture) c’est logique.
Oui c’est la meilleure motivation pour mon fils Marc donc c’est pour ça que je fais le mien “ programme d’amis et planification hebdomadaire (oui, vous devez envoyer des messages / appels téléphoniques pour planifier 5-6 invitations par semaine- in organisation et planing de » ministre » que c’est à vous – maman de gérer….Souvent, les parents n’ont pas le temps / la motivation pour jouer avec leurs enfants à la maison (moi j’ai ce temps et motivation et mon mari aussi joue avec les enfants juste pendant les week-ends! Ils adorent jouer avec lui même bien plus que avec moi 🙂
Je connais 11 enfants de sa classe maintenant ( et on continue à faire Nouvaux copains toujours ) et leurs parents biensure .
Je sais t’es bien que parfois jouer avec eux des jeux sociaux peut parfois être très ennuyeux pour les adultes et nous, en tant que parents, on veut parfois juste se reposer, je sais tout cela! Mais ça n’est pas thème de cet article ….
J’ai une chance que maintenant Marc peut jouer un peu seul ( avec un copain ou un copine) sur mon surveillance mais là après 2 ans il y a des moments que je peut les lesser juer LEGO un peut ou playMobiles entre les enfants mais ça ce n’était pas si évident il y a 2 ans … et oui, j’invite parfois 2 de ses meilleurs amis (garçons) à dormir à la maison pour que nous puissions faire des soirées pyjamas 😉 et danser ou juer « 1,2,3 soleil « , je vais vous dire que c’est beaucoup de boulot / je suis devenu un animatrice presque professionnel ….tien un future bulo à clubMed? ( pour ma retraite )…
Mais ça vaut le coup : vous pouvez pas d’imaginer ce que je ressens cette année quand des enfants que je ne connais pas encore de sa classe viennent me voir et me demandent: » tu est Maman de Marc. S’il te plaît, peux-tu m’inviter à manger avec Marc? je suis son ami « … et donc – je demande à mon fils Marc » tu connais ce garçon tu veux l’inviter à la maison? « Et son plaisir de me dire -« oui je veux oui il joue avec moi à l’école …. ou alors l’autre jour « maman peux-tu inviter ce garçon … etc … » C’est vraiment un sentiment très agréable…. Beaucoup de travail mais tellement cool! 🙂C’est un long chemin mais ça vaut le coup! Comme j’ai déjà dit qu’il m’a fallu 2 ans pour retrouver la socialisation de Marc après son arrêt cardiaque soudain.
J’ai commencé avec 2 meilleurs amis – les invités régulièrement à la maison (pendant 2-3 heures) – le week-end. J’invite toujours ( sauf anniversaire) un seul copain à la fois …. c’est plus facile à gérer et c’est mieux pour Marc. Ensuite, j’ai commencé à inviter des amis à manger avec Marc à la maison pendant les déjeuners (c’est parce que moi qui organise tout ce que je vais à l’école en emmen les enfants / je les fait à manger ensemble et jouer – et je les ramene à l’école après ) – les parents n’ont qu’à dire à l’école qu’ils me donnent la permission de prendre leurs enfants pour le déjeuner (donc pas trop de problèmes pour les autres parents et aucun problème pour leurs habitudes quotidiens).
A ce jour je suis en fait: au niveau 3 déjeuners par semaine (chaque fois que j’invite un seul ami) Et chaque Vendredi soir – très souvent il joue avec des amis (après l’école) Et 2 enfants pendant 4 heures invités à jouer chaque samedi et dimanche!
Oui emplois de temps de ministre….Donc 5- 6 amis par semaine! C’est un vrai travail je gère clubKids ou clubMed à la maison mais ça en vaut la peine! Et si vous le savez, comment Marc est heureux d’avoir tous ses amis!

Voilà mon livre « Marc L’invincible » est désormais en ligne et disponible* à l’achat dans la boutique Kindle: ( en français)
https://www.amazon.fr/dp/B07Y34WPXQ
« Marc L’invincible: L’histoire vraie d’une récupération remarquable, après arrêt cardiaque et lésions cérébrales anoxiques », est désormais disponible en livre broché dans la boutique Amazon. Les lecteurs peuvent l’acheter:
https://www.amazon.fr/dp/B07Y4KC5S1
Here is my book « Marc L’invincible » is now online and available * for purchase in the Kindle store: (in French)