As a lot of parents with injured child I have heard about CBD and TCH oils…
so what I did: I found who is doing scientific studies about… I had a chance Israel is doing the most advanced studies about canabidols oils for CP and autisme.
So we met dr Blumkin only once for my son consultation in February 2017… before results of her study for cp was published…. my son was absolutely not candidate for Cannabidiol (CBD) oil. We have to consider Cannabidiol (CBD) and TCH as any other pharmaceutical Médecine so it can have side effects as any other medications… so for each case it must be taken in account for benefits/ possible side effects.
So hire contact if somebody needs it:
Lubov Blumkin MD
Head, Pediatric Movement Disorders Clinic
Pediatric Neurology Unit
Metabolic Neurogenetic Clinic
Wolfson Medical Center
Holon, Israel
Tel. +972-35028458
lubablumkin@gmail.com
She did this study:
For cp
Hire Israel study published : « Medical cannabis in children with complex motor disorders »:
Honestly I don’t personally liked TheraSuit we tried long time ago in Spain for Marc ( he hated that it was tearing him all diferent ways and didn’t supported it more than 3 minutes ) ….may be I didn’t tried too long enough but it was all as our experience with suits for naw….
I never tried yet for my son Marc because he has electrical suplimental pathways in his heart (wpw syndrome) I wasn’t convinced that it was safe to try it … next September 2018 I will go in Italy to check his WPW and if it’s ok after 5th operation and we get Professor Pappone agrément so may be I will try it….this winter
So I can give just informations about I can’t testimonials about haw it works ok;)?
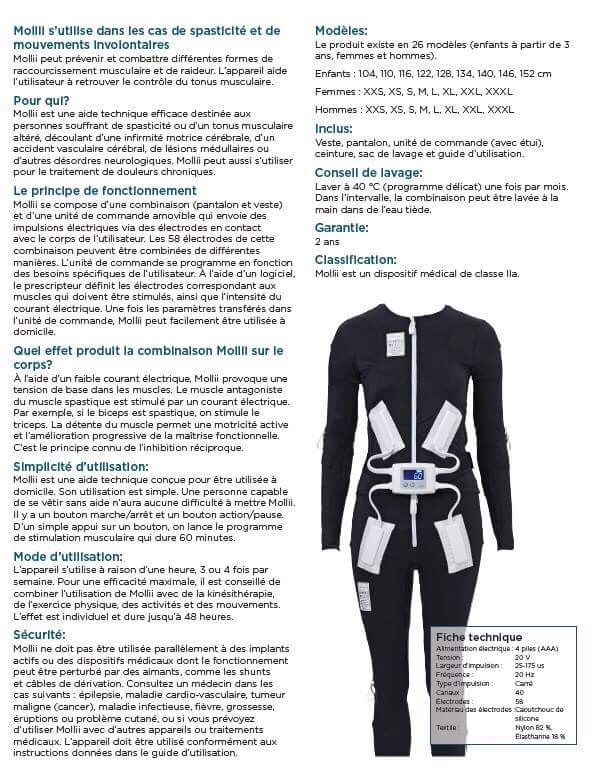
« The Mollii Suit is a new assistive device developed by Inerventions, a Swedish company, that can “relax spastic, tense, and aching muscles.” The company was started by Mollii inventor Fredrik Lundqvist in 2009. According to their website, Mollii is currently being used by people with cerebral palsy, stroke, spinal cord injury, acquired brain damage, and neurodegenerative conditions. Inerventions mission is, “creating opportunities for active movement and functional improvements, and providing everybody with the chance to live a dignified and active life.
How does it work?
The suit has 58 electrodes which can be combined in various ways. Mollii has a control unit which is individually programmed for each user. The person prescribing Mollii uses a computer program to adapt the active electrodes and the intensity (which muscles are to be activated by means of current). The settings are then saved in the Mollii control unit, making it simple for the device to be used at home.
Mollii uses low level electric current to produce basic tension in the musculature. The current stimulates the antagonist to the spastic muscle. If, for example, the biceps is spastic, the triceps is stimulated which in turn makes the biceps relax. Relaxing the muscle enables active movement and a gradual improvement in function. The physiological mechanism is called reciprocal inhibition. »
I post the exact words of Kristal Carlson mother of Eden:
“On February 29, 2016, our 23 month old daughter, Eden, got through a baby gate, pushed open a heavy door, and got into our swimming pool. The water was cold – about 45-50 degrees, not freezing. She was in the water 5-15 min. When I found her, she was cold and unresponsive. I immediately started CPR. Paramedics took over and then emergency room nurses. Eden had approximately 100 minutes of CPR and 17 shots of epi to get her heart beating again. The efforts of the paramedics, nurses, and doctors were truly heroic. Once stable, she was life flighted to Arkansas Children’s Hospital that evening. Her body was kept cold for 72 hours, and then they slowly warmed her up. Her kidneys and liver were not functioning and her blood was very acidic, but slowly she started to improve. She was extubated 11 days post accident and moved out of the PICU 13 days post accident. She spent 5 weeks total in the hospital. She suffered an anoxic brain injury mostly affecting the deep gray matter of her brain. She was fed by g tube and was in a vegetative state, unable to communicate or move her body with purpose. She was on baclofen for tone and propranolol and clonadine for neurostorming. We were told there was nothing more that mainstream medicine could do for her. We would have to ‘wait and see’ how she recovered. During this time we gave her double doses of fish oil, an herbal supplement called Vital Guard Supreme, and we diffused frankincense essential oil around her and rubbed it on the back of her neck several times per day.
We contacted Dr. Harch out of New Orleans a couple of weeks after Eden was released from the hospital. Approximately 8 weeks post accident, we started giving her normobaric oxygen, 3 L twice per day for 45 minutes by nasal cannula under Dr. Harch’s direction. Immediately after the first dose we saw a reduction in tone, she stopped squirming her severely postured body, and her eyes became more clear and focused. During the 2.5 weeks of this treatment at home, she began smiling and laughing, tracking with her eyes, saying about 10-15 words she recalled from before her accident, she regained her swallow and stopped drooling, started holding her head up, had a reduction in tone, and she started trying to use her hands to swipe at toys and grab. At 10.5 weeks post accident Eden started hyperbaric oxygen therapy (HBOT) under Dr. Harch’s care in New Orleans. After 4-5 treatments she could recall animal sounds, recall how to count to five, used her hands more, and she started trying to sit up.
During the two months we were in New Orleans Eden completed 40 HBOT sessions at 1.3 ATA on compressed room air. She had physical therapy twice per week. She had her g tube removed because she no longer required it. I weaned her from all prescription medication, as she no longer displayed a need for it. Almost all tone left her body. She could move her body with purpose. She could sit independently, scoot, pull herself to stand, and she started taking shaky steps by the end of her treatment. She regained all her vocabulary and speech abilities, plus more than she was capable of before her accident. She had a miracle recovery.
Her MRIs after 40 HBOT sessions were read as ‘normal’.
Today she has had over 100 HBOT sessions. She now has a soft chamber at home, and we continue treatment under Dr. Harch’s care. She walks well with assistance, and in all other ways she is a typical 4 year old child. Her cognitive abilities and speech are normal. She is always improving. Other than HBOT, she has attended the Plasticity Center in Orlando for one week. She has continuing occupational therapy 3 times per week. She has physical therapy 3 times per week – once in clinic, once in a pool, and once on horseback.
She is learning to swim”
Case of study:
Anoxic injury (near drowning) 2-year-old Eden Carlson’s road to recovery has defied the odds and is possibly the first medical case of its kind.case of study published:
Je poste les termes exacts de Kristal Carlson, la mère d’Eden:
“Le 29 février 2016, notre fille de 23 mois, Eden, a franchi une barrière de protection pour enfants, a ouvert une porte lourde et est tombée dans notre piscine. L’eau était froide – entre 7 et 10 DC, elle n’était pas gelée. Elle est restée de 5 à 15 minutes dans l’eau. Quand nous l’avons trouvée, elle était froide et ne répondait plus. J’ai immédiatement entrepris la réanimation cardio-pulmonaire. Les aides-soignants puis les infirmières de la salle d’urgence continuèrent. Eden a subi approximativement 100 minutes de réanimation cardio-pulmonaire et 17 chocs électriques pour que son coeur se remette à battre. Les efforts des aides-soignants, des infirmières et des médecins furent vraiment héroïques. Une fois son état stabilisé, elle fut amenée, en vie, par avion à l’hôpital pour enfants de l’Arkansas le soir même. Son corps a été refroidi pendant 72 heures, puis doucement réchauffé. Ses reins et son foie ne fonctionnaient plus et son sang était très acide, mais graduellement, elle commença à faire des progrès. Elle a été détubée 11 jours après l’accident et sortie des soins intensifs pour enfants 13 jours après l’accident. Elle a passé 5 semaines en tout à l’hôpital. Elle souffrait d’une blessure anorexique du cerveau affectant principalement la matière grise profonde de son cerveau. Elle était nourrie au moyen d’un tube et était dans un état végétatif, incapable de communiquer ou de se mouvoir volontairement. On lui donnait du Bacloféne pour son « tone » et du Propranolol et de la Clonadine pour son attaque cérébrale. On nous a dit que la médecine traditionnelle ne pouvait rien faire de plus pour elle. Il nous fallait attendre et voir comment elle allait récupérer. Pendant ce temps, nous lui avons donné une double dose d’huile de poisson, un complément de plante appelé Vital Guard Supreme, et nous avons diffusé de l’huile essentielle d’encens autour d’elle et en avons frotté l’arrière de son cou plusieurs fois par jour.
Nous avons contacté le Dr. Harch à la Nouvelle Orléans quinze jours après la sortie d’Eden de l’hôpital. A peu près, 8 semaines après l’accident, nous avons commencé à lui donner de l’oxygène normobare, 3 L deux fois par jour pendant 45 minutes à l’aide d’une canule nasale sous la supervision du Dr. Harch. Immédiatement après la première dose, nous avons constaté une réduction de « tone », elle a arrêté de tortiller son corps qui était en très mauvaise position, et ses yeux devinrent plus clairs et concentrés. Pendant ces 2.5 semaines de traitement à la maison, elle a commencé à sourire et à rire, suivant des yeux, disant environ 10-15 mots dont elle se souvenait avant son accident, elle pouvait avaler à nouveau, et s’arrêta de baver, elle commença à redresser sa tête, eut une réduction de « tone », et a commencé d’utiliser ses mains pour saisir et déplacer ses jouets. 10.5 semaines après l’accident, Eden a commencé une thérapie d’oxygène hyperbare (HBOT) par le Dr. Harch à la Nouvelle Orléans. Après 4-5 traitements, elle pouvait se souvenir de bruits d’animaux, compter jusqu’à 5, mieux utiliser ses mains, et commencer à essayer de s’asseoir.
Pendant les deux mois que nous avons passé à la Nouvelle Orléans, Eden subit 40 sessions de HBOT à 1.3 ATA dans un caisson hyperbare.Elle avait une ergothérapie deux fois par semaine. Son tube lui a été enlevé car elle n’en avait plus besoin. Je lui ai enlevé tous les médicaments faisant l’objet d’une ordonnance car elle n’en montrait plus le besoin. Presque tout le « tone » avait quitté son corps. Elle pouvait se mouvoir intentionnellement. Elle pouvait s’asseoir indépendamment, se mouvoir, se dresser, et commençait à entreprendre des pas incertains à la fin de son traitement. Elle a retrouvé tout son vocabulaire et pouvait parler encore mieux qu’avant son accident. Elle a récupéré par miracle.
Son IRM, après 40 sessions de 40 HBOT était normal.
Jusqu’à aujourd’hui, elle a eu plus de 100 sessions de HBOT. Elle a maintenant son propre caisson d’appoint à la maison et nous continuons le traitement sous la supervision du Dr. Harch. Elle marche bien en étant assistée et, pour le reste, elle se comporte comme une enfant de 4 ans. Ses capacités cognitives et son langage sont normaux. Elle continue à progresser. Outre le HBOT, elle est allée au Centre de Plasticité d’Orlando pendant une semaine. Elle continue de l’ergothérapie 3 fois par semaine. de la physiothérapie 3 fois par semaine, une fois en clinique, une fois en piscine et une fois à cheval.
Elle apprend à nager.
Cas d’étude:
Blessure anorexique (presque noyade) histoire de l’enfant de 2 ans, Eden Carlson, qui a défié tous les pronostics et est probablement le premier cas médical de ce type dont le cas d’étude a été publié:
1) What about official sientific researchers about Feldenkrais and Anat BanielMethod?
So as usual for any alternatives therapies I did my own » research » ….why to make any research about official scientific studies for alternatives ( not recognized by mainstream medicine) therapies? It’s simple: or therapies has at least some scientific studies that’s means for me that they want to be recognized / accepted by mainstream medicine and they are doing efforts for their patients ( in order to be payed by insurance) and not directly from pocket of parents/ patients….
So on link you can find what » mainstream medicine » thinks about both therapies:
But I want to say I send them my « scientific findings » about Feldenkrais by mail:
pencru@exeter.ac.uk
will see if they will answer me?
So what I found:
1)I have found it. It is interesting: Feldenkrais Method (FM) : 2 links on scientific studies so for this method we have some efforts in order to be recognized….. obviously not yet enough for mainstream medicine:
But for mainstream Medcine 2 links I gave is not not enough :
2)Anat Baniel Method – ( no links ) sorry I didn’t found any published research ….she obviously not interested in any scientific studies…..or she has to recognized that studies for Feldenkrais Method (FM) is enough for her method because it’s same basis ???? So than again what is the difference than in methods?
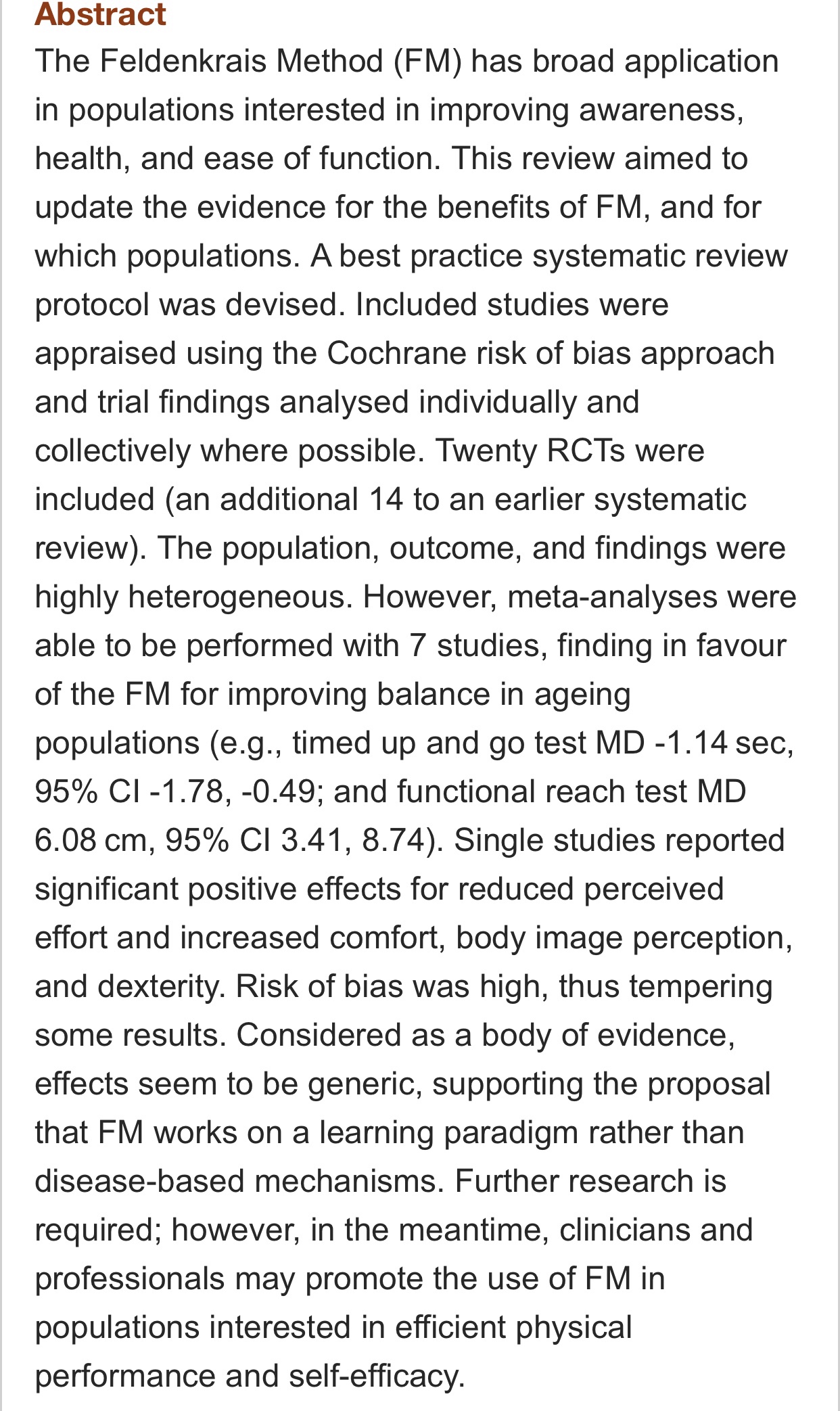
Hire you can find a good summary of the most recently published studies on the Feldenkrais Method in the editorial of the Feldenkrais Journal. It mentions the systematic reviews that I have mentioned before, as well as research published after those reviews:
It’s worth quoting in full a portion of that editorial: « One ongoing challenge in investigating the outcomes of the Feldenkrais Method is that it is very difficult to ‘blind’ trials for practices like Feldenkrais (for example, for participants to not know whether they are receiving the “intervention” or not). Even with sham interventions, participants will often be able to guess fairly accurately which is the real intervention and which is the sham (Licciardone and Russo 2006). This lack of blinding is one of the reasons that the evidence in Feldenkrais outcome studies frequently receives a lower level of evidence rating. Buchanan draws on work by Mehling, DiBlasi, and Hecht (2005) to suggest ways that this risk of bias can be dealt with in studies of practices like the Feldenkrais Method. »
With this in mind, I wonder if « objective » evidence for the efficacy of the method may be strengthened with fMRI and other brain activity studies; I have only seen one by Verrel et al (2015), which is mentioned in that editorial. I would be interested in hearing more about work done in this domain????? 😉
I will not put the name of our Feldenkrais practioner in this article because this article is about ONLY MY OWN feelings and reflections only in prosess to find best and most confortable way for us as family to use for him such kind of therapie…
So First I read a book : the Norman Doidge book, « the brain’s way of healing », in one of chapters he is talking about Feldenkrais method and haw Anat Baniel studed with Moshe Feldenkrais….
So I started to search about both of this methods.
I was adviced by a lot of parents about ABM
( it’s obvious Anat Baniel Method is more popular in USA….)
But my question was:
What is the difference between Dr. Feldenkrais’ Method and the Anat Baniel Method? Logical question isn’t it?
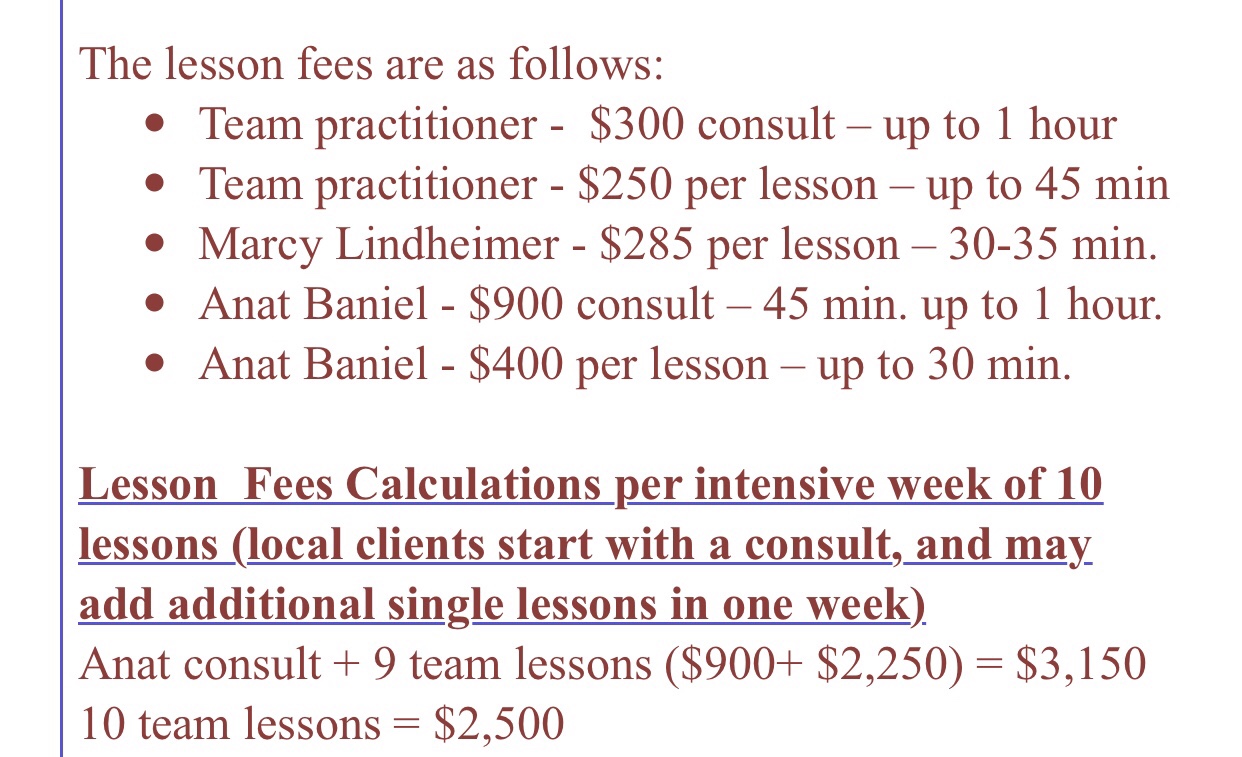
As well as the prices difference ?
As all parents I know haw much it cost all therapies ( haw much we need to travel in order to make our children’s progress)….
So what I did :
I asked prices for 3 centers of ABM ( you can find their answer from Anat center on photo)
And I asked a prices of Feldenkrais practitioner (in GRENOBLE in france in town i live and i found that to get personalized privat treatment at my own home is the best and less expensive way so that’s why I chooses Feldenkrais) it seems Fire me more much more better than to go somewhere for expensive intensive therapy.
So Feldenkrais practitioner private lessons price:60€/ per hour .
I think ( and it’s only my opinion ok?) comparing to ABM prices it’s more reasonable and more confortable option let’s say and just at my home I don’t need to travel and to pay accommodations and tickets.
Yes may be ABM is more specific to children but Anat Baniel is over rated and over priced even if her practitioners are great. This is my opinion.
I am trying to be honest with myself and with others parents who reading my posts … they are my public … because we have injured children’s ….
so I may somtimes not « usual for you » and to direct ok take it like my Russian soul ok? I am direct I am Russian tank in order to save my child…..
So what may be not all parents know that there was in a Court’s because of the fact that this … Anat Baniel studied the Feldenkrais Method under Dr. Moshe….. she was juged for I don’t know haw to name it? Don’t wanted to use hard word but me it’s bother me ….( she gained by the way she must have very good avocat)….:)
Yes Anat was trained in 1977
And she was Feldenkrais practioner till 1987 (10 years before they « separated »)…
As I said I meant that both methods in fact is the same method ….. for me it’s looks like this ?
Just I don’t find prices of ABM not fair in comparison ho original method Feldenkrais she was thought originally and she is not the only one trained by Moshe….( I have the right to think what I want about price policy ;)…
And don’t forget Moshe trained personally 323 people !!!!!
One of them in New York for example ….
I think one of them ( traind personally by Moshe in New York Feldenkrais center:) you can check it : David Zemach-Bersin
This was my point:
Dr Feldenkrais trained personally three groups of people to be teachers in the Feldenkrais Method. The first group in 1969, was trained in Tel Aviv,13 people. The second group graduated 60 teachers in the USA in 1977.
In 1983 Feldenkrais managed to train his third group of teachers, 250 in number. These teachers under Dr. Feldenkrais’ instruction, founded the Feldenkrais Guild in the USA.
But honestly do you really think she invented her method or changed it so profoundly that it worth so big difference in price?
very good marketing 👏 bravo
I prefer to stay with original Feldenkrais Method and honest prices 😉 and feelings….
Why I think about this I just think that a lot of parents never go so deeply in their research…..before starting any therapies 😉
It’s dosent meant that ABM is not good method but honestly 900$ for Anat Baniel personal consultation 45minutes????
So I don’t like when I see such kind of thing I I just want to tell parents)….
What I am trying to tell hire it’s « big picture » take a perspective 😉
Anat chagring more than Professor Pappone 😉one of the best cardiac chirurgien of the world ( for his consultation he is Professor he is doing 5-6 operations on heart per operations day and he is the one invented method for incurable before him Brugada syndrome….) no it’s not only matter of location ( like California) …. it’s only my feelings….
If you think she deserves 900$ for consultation …..and it’s ok fo you so go with it…..
Dr Pappone is one of the most famous cardiac ( in fact Rythmologue doctor of this planet )….and charging 450€
Anat 900$….so
It’s your choice….if you think it’s honest price…..
My son has had 5 heart operations ( it’s ablation of his WPW) wolf Parkinson’s wight syndrome. It’s a mainstream operation but in France 2 doctors couldn’t do this operation successfully -they attempted 3 operations here in France.
I had to find best doctor in world ( in Italy) he is professor and researcher in this domain : Rythmologie and his heart hospital has other techniques- 5 catheters ablation, named
« Pappone ablation technique » so he was finally successful! There isn’t a hospital in the world that doesn’t use technology designed by Dr. Carlo Pappone
( I payed 450€ for consultation with him = one of the best rhythmologtist Dr Papponne he is operated my son for his heart syndrome he is chirurgien one of the best on heart fir thachicardias and arytmias…. sorry he is just 5 head taller in knowledge and education than Anet … Professor Pappone has more than than 200 scientific studies and publications more than 100 tousends hearts operations …. and he is taking 450€ for consultation ! With cardiogramme and ultrasound of heart included in price!)
So what I think about method Feldenkrais:
First : I like it it’s different type of physical therapy I don’t know haw explains better it’s just diferent… I felt it on my own body so can testimonial this. But my question in my « very logical head »was: if it was studed by scientific means? Lol 😂
I see just some gains in Marc lately with Feldenkrais’ Method just some more openings of both hands
May be a bit more energy… and balance….but I think it’s must be long therapy so I will continue once a week for next year will see the results and I will tell you than of cause …. but as usual for my son it will be mixture of results ( because we are doing not only one but severa therapies at the same time…)
Feldenkrais is extremely popular in some communities (e.g., dance), and its participants are strong believers in the approach. The foundation of the approach is based on knowledge/beliefs about the nervous system in the mid-20th century regarding sensorimotor education and the best approach to teaching new or « more efficient » movement patterns. This basis badly needs to be updated based on current knowledge of the nervous system, especially motor learning and systems neuroscience.
Hi everybody I get permission to shere this informations from LEAH RODAS, Administrator and central coordinator for the Center of dr Dr. Richard Neubauer’s ( may be not everybody knows but he is one of first doctors who started to treat neurological conditions with Hbot.) Dr. Neubauer’s pioneering work with hyperbaric oxygen and the potentially recoverable brain led to the development of the first medical center in the world to focus on the role of HBOT in aiding the recovery of patients from stroke, coma, traumatic brain injury, cerebral palsy, and anoxic encephalopathy.
But it’s for carmiopathy case ( so stem cells injections was done near heart zone where located the problem of patient)….
Day 1 lecture 7 Arun Mukherjee:
Stem cells +Hbot ( sorry I can’t openly share this dr Arun Mukherjee PowerPoint presentation ) but you can contact me by my mail and ask privately send it to you.
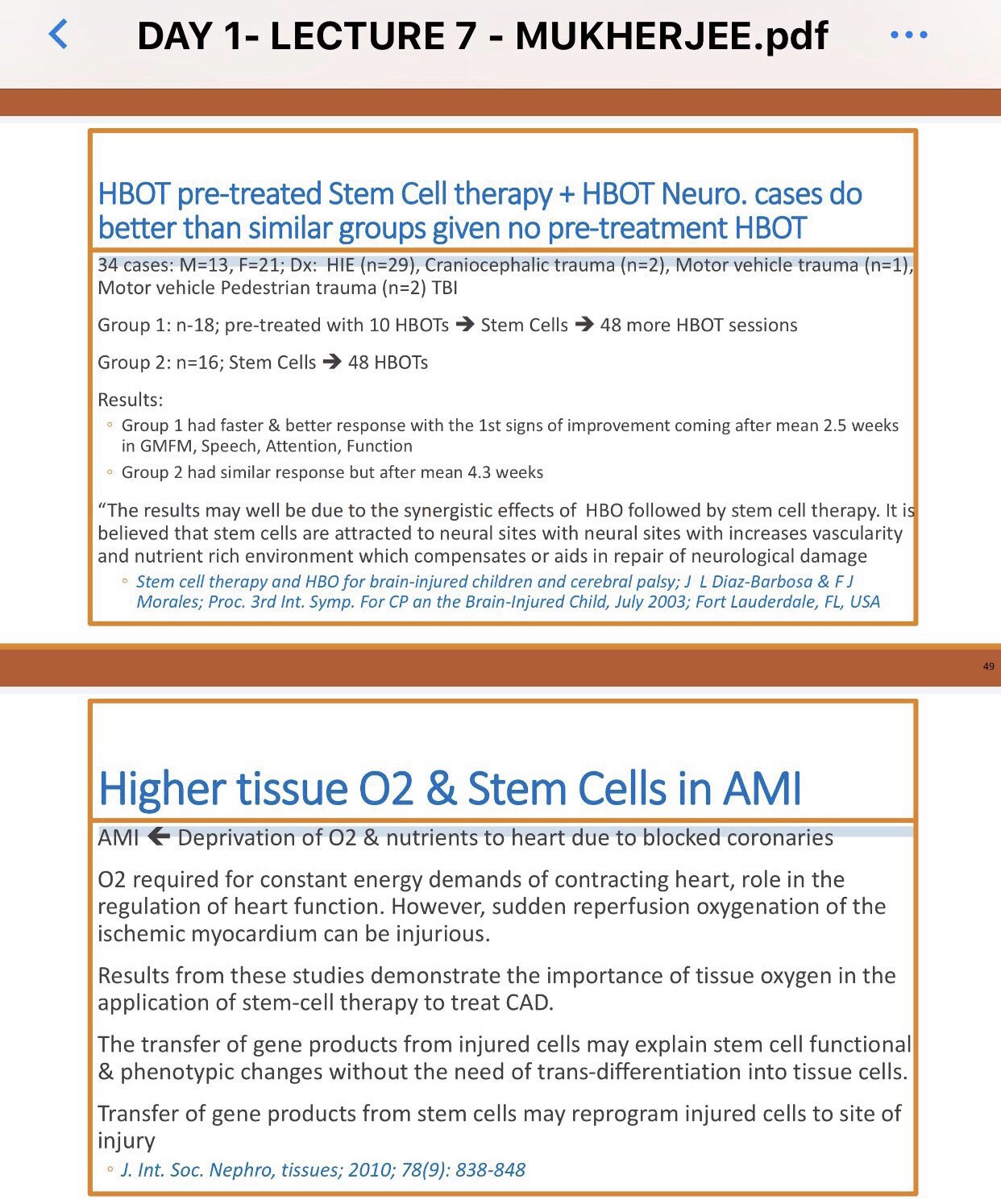
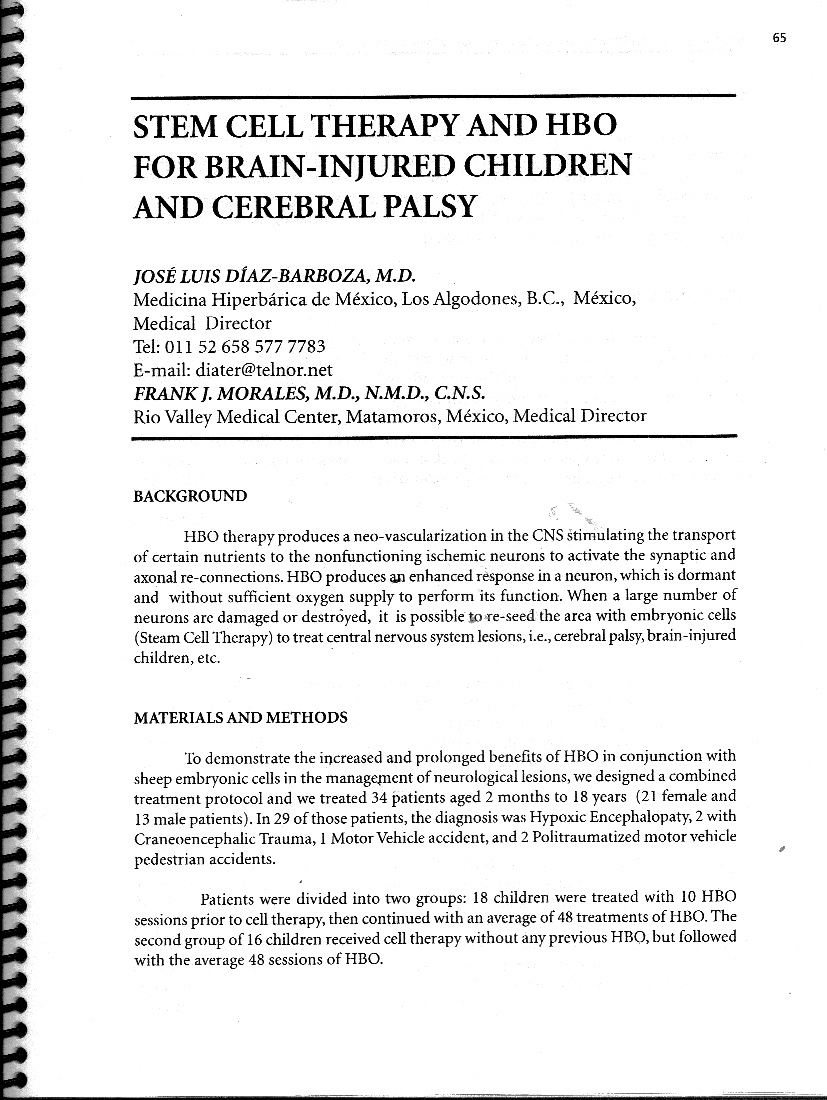
So here on photos: presentation of : “Stem cells therapy and HBO for brain-injured children and cerebral palsy “ ; J L Diaz – Barbosa & F J Morales; Proc. 3d Int. symp. For CP and the brain-injured child, July 2003, Fort Lauderdale, fl,USA)
I think first : it’s old presentation 2003…. and they where using embryonic stem cells !!!! So honestly this kind of stem cells can grow to teratomas…
But in presentation of dr Arun Mukherjee he is talking about MSC ( if I understood well ? Allogenic Wharton Jelly)
So why he used such kind referral in his 2018 presentation ? With embryonic sheeps cells? For me it’s just incomprehensible….
So I asked Mr Fogarty and Dr Harch if I will have rights to share lecture slides in pdf of sombodys presentations during Denver Hbot 2018 conference on my blog and I don’t get any answer.
But I wanted to say what I think about this from parent point of vue:
Not all parents can go to Denver conference ( it’s simply expensive for example to go from France I need tickets for plane and hotel to stay as well as to pay fee for attend conference) budget about 3000$? For 3 days if I go alone and just live my hasbend to take care of Marc during 3 days without going to job 😂 not reasonable I know
Yes I can try to watch conference on life ( if I pay ) but it’s night time in France where I live during lifestream of conference….i have to stay up 3 nights in order to see all conference? 😂 not reasonable either….yes we can pay lifestream for 295$ ( just haw we stay 3 nights up to see it?)
I think PowerPoint presentations of lectures can give at list some informations to parents.
So when you read PowerPoint slides of any presentations please don’t forget that generally for such kind of presentation :
Only Minimal text: key words used only as a means emphasize and highlight points to the audience the oral presentation is very important …so…Because slides in no way provide or capture the complexity of ideas that was presented, you have to keep this in your mind that without author interpretation of what is on those slides you can misunderstand something or simply not get enough informations.
Still I think that to share such informations with public ( parents of children’s who is choosing to make Hyperbare treatments which is not recognized by fda for neurological conditions) is our rights especially that parents was permitted this year to attend Hbot 2018 Denver conference.
May be if the deciders of hbot conference will let parents watch conference researches and presentations for FREE for parents and patients with conditions doctors discussing on conference will be next step? ( we can send you official papers and administrative attestations from doctors which confirm our child conditions as proof)? And I think parents pay already very much from their pocket for hbot ( because it’s not recognized and not payed by insurance) do we really need to pay also for get knowledge about hbot latest research ?
In fact it’s parents who taking steps and deciding if they apply hbot to their children’s condition ( yes with help of doctors specialized in hbot) but still they have a rights to know all available scientific informations.
I really like and respect all authors rights, however, it is not my intention to harm so for parents who want be informed and who
wants to recive PowerPoint presentations : please contact me in private by mail.
I think such a gesture would help us build on the important ideas, research, and evidence presented at conferences, and of course allow for better citation of these ideas.
I have listen a lot of incredible conferences where the presentations have been innovative, robust, and valuable; I worry that the ideas of researchers at hbot 2018 Denver conference are not as accessible, and reliable as they deserve to be especially for parents of children’s this doctors treating…
How do you think we can ensure the valuable knowledge presented at Hbot professional conferences can be shared accurately and reliably to parents ?
in an ideal world, everyone would be presenting a research paper. However, parents also must be aware that not all the presentations are research-based…..but anyway I don’t think they should all be research-based. We also can learn a lot from the “here’s what we did at my hbot clinic and here what it was as results » this types of presentations….
***This article gives only my views on topic of Publication Policy Hbot Denver conférence 2018
(Fr):
Ai-je le droit de partager les diapositives de lecture en PDF de la présentation de quelqu’un pendant la conférence de Denver HBOT 2018 sur mon blog ?
Aussi ai-je demandé à Fogarty et à Harch si j’avais le droit de le faire non seulement sur mon blog mais aussi sur Facebook ? Je n’ai pas encore la réponse.
Mais je voudrais dire ce que j’en pense du point de vue des parents.
Ce n’est pas tous les parents qui peuvent aller à la conférence de Denver, cela coûte cher en avion, hôtels et en billet d’entrée. Le budget est de l’ordre de 3 000$. De plus, je ne peux pas laisser mon mari pendant 3 jours seul avec Marc alors qu’il doit travailler😂 je sais que ce n’est pas raisonnable.
Oui, je sais que je peux voir cette conférence, si je paie, en direct mais c’est la nuit en France. Il faudrait que j’y passe trois nuits pour toute la conférence 😂 ce n’est pas raisonnable non plus…ou nous pouvons payer 295$ pour la suivre en continu et y passer 3 nuits.
Je pense qu la présentation de lecture PowerPoint donne au moins quelque information aux parents..
Pour la lecture de PowerPoint n’oubliez pas que:
Pour un texte minimum: des mots clé sont utilisés pour accentuer et souligner certains points à l’auditoire, la présentation orale est très importante …ainsi…par ce que les diapositives en aucune façon ne peuvent capter ou fournir la complexité des idées qui sont présentées,vous devez vous souvenir que, sans la présentation de l’auteur, vous ne pouvez pas bien comprendre ou ne pas avoir assez d’information.
Je pense encore que partager l’information avec les parents d’enfants ayant choisi le traitement Hyperbare, qui n’est pas reconnu par la FDA pour des raisons neurologiques, est notre droit d’autant plus que les parents ont été admis à cette conférence sur le HBOT à Denver.
Il se peut que s’il était décidé de laisser les parents assister à cette conférence gratuitement et en pouvant discuter avec les médecins, sous conditions, serait la prochaine étape? Nous pouvons envoyer des documents officiels et des attestations de médecin qui confirment l’état de nos enfants comme preuve.? Les parents dépensent déjà beaucoup d’argent pour le HBOT car il n’est pas reconnu donc pas remboursé par l’assurance.En plus, devrions nous payer aussi pour être informés des dernières recherches sur le HBOT ?
En dernier lieu, il appartient aux parents d’appliquer le HBOT à leurs enfants avec l’aide des médecins spécialisés, mais ils doivent avoir accès à toute l’information scientifique disponible.
J’aime et respecte réellement les droits d’auteur cependant il n’est pas dans mon intention de porter préjudice aux parents qui veulent être informés et recevoir une présentation PowerPoint: contactez moi en privé par mail.
Je pense qu’une telle attitude aidera à bâtir d’importantes idées sur la recherche et mettra en évidence ce qui est présenté à la conférence et permettra une meilleure présentation de ces idées.
J’ai écouté un nombre incroyable de conférences à la présentation innovante, solide et valable, je regrette que les idées des chercheurs à la conférence de Denver HBOT 2018 ne soient pas accessibles comme elles le méritent aux parents dont les enfants suivent ce traitement…
Comment atteindre cet objectif ?
Dans un monde idéal, chacun présente un document de recherche. Cependant, les parents doivent savoir que tous les documents de présentation sont basés sur la recherche….mais je ne pense pas qu’ils doivent être tous basés sur la recherche. Nous pouvons aussi beaucoup apprendre de l’expérience du style: » Voici ce que nous faisons dans notre clinique HBOT et voici les résultats. » ..
***Cet article donne seulement mes sentiments sur la politique de publication de la conférence de Denver sur le HBOT
I have to say : during our experience I did mistakes as well: one of them: I agreed to botox injections…..( I didn’t know much back in February 2016 one month after Marc anoxic injury….so I agreed to Dr experience…. what a fool I was….) ….so 1 time Botox experience horrible … painful without visible results in
2 months! But it was done for my son while his local anesthesia didn’t worked …so he was traumatized for 1 year with seringues after Botox injections…. ( even take a simple blood test for him was very very difficult more than 1 year after this terrible experience ….).
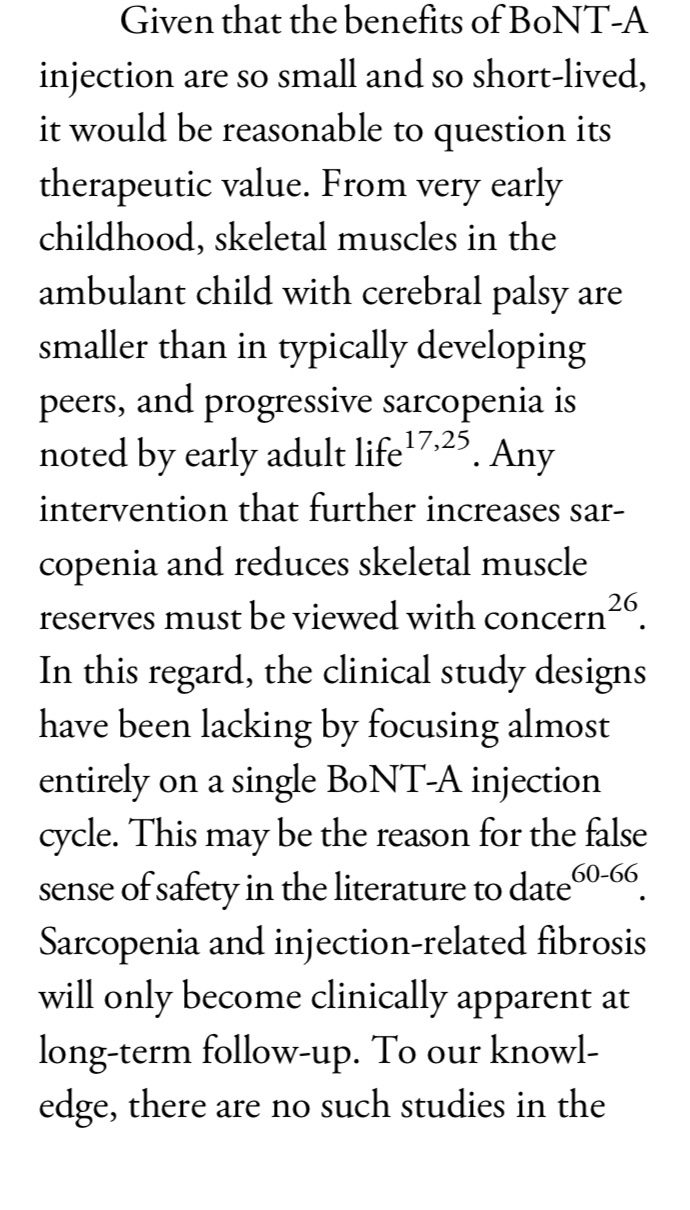
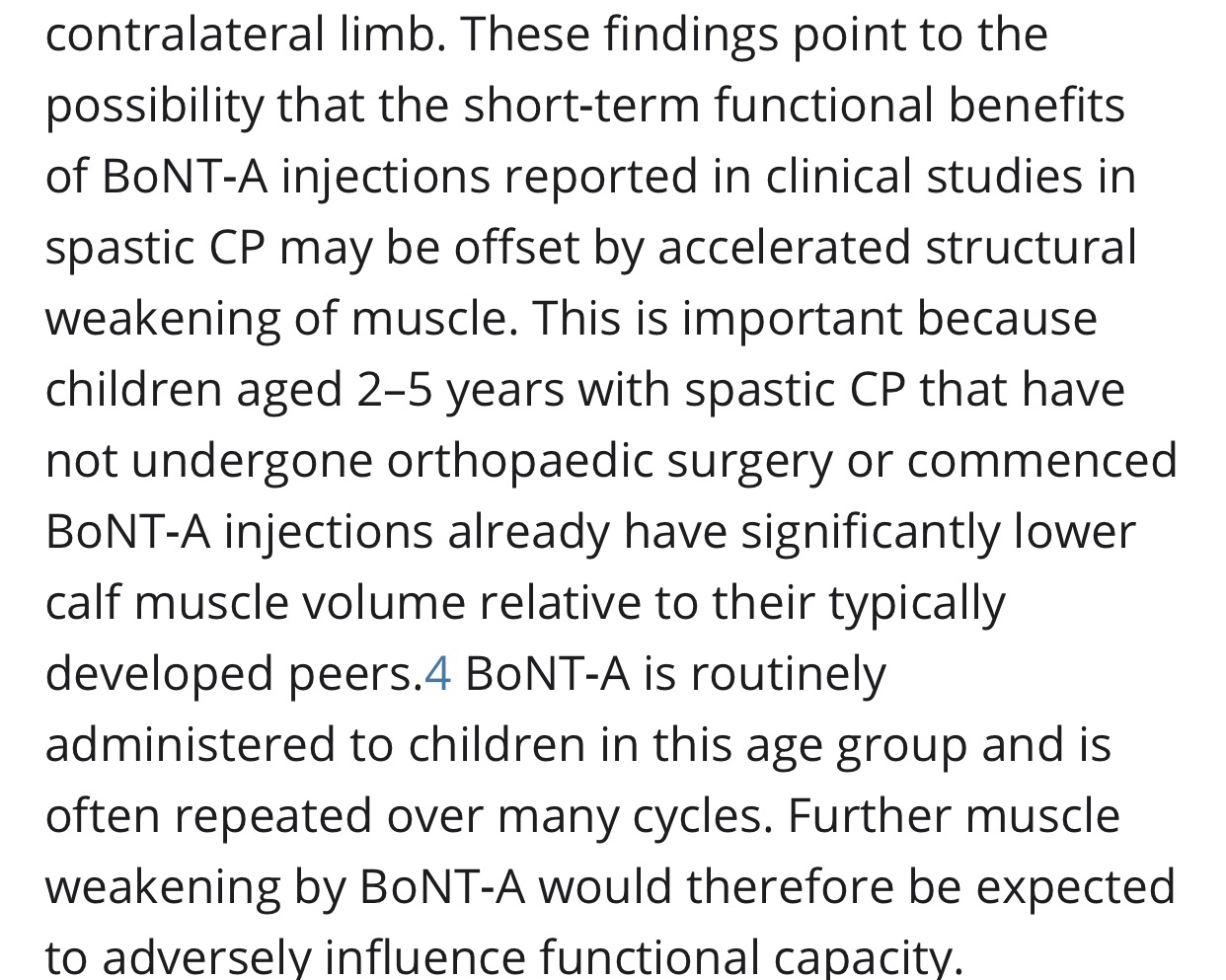
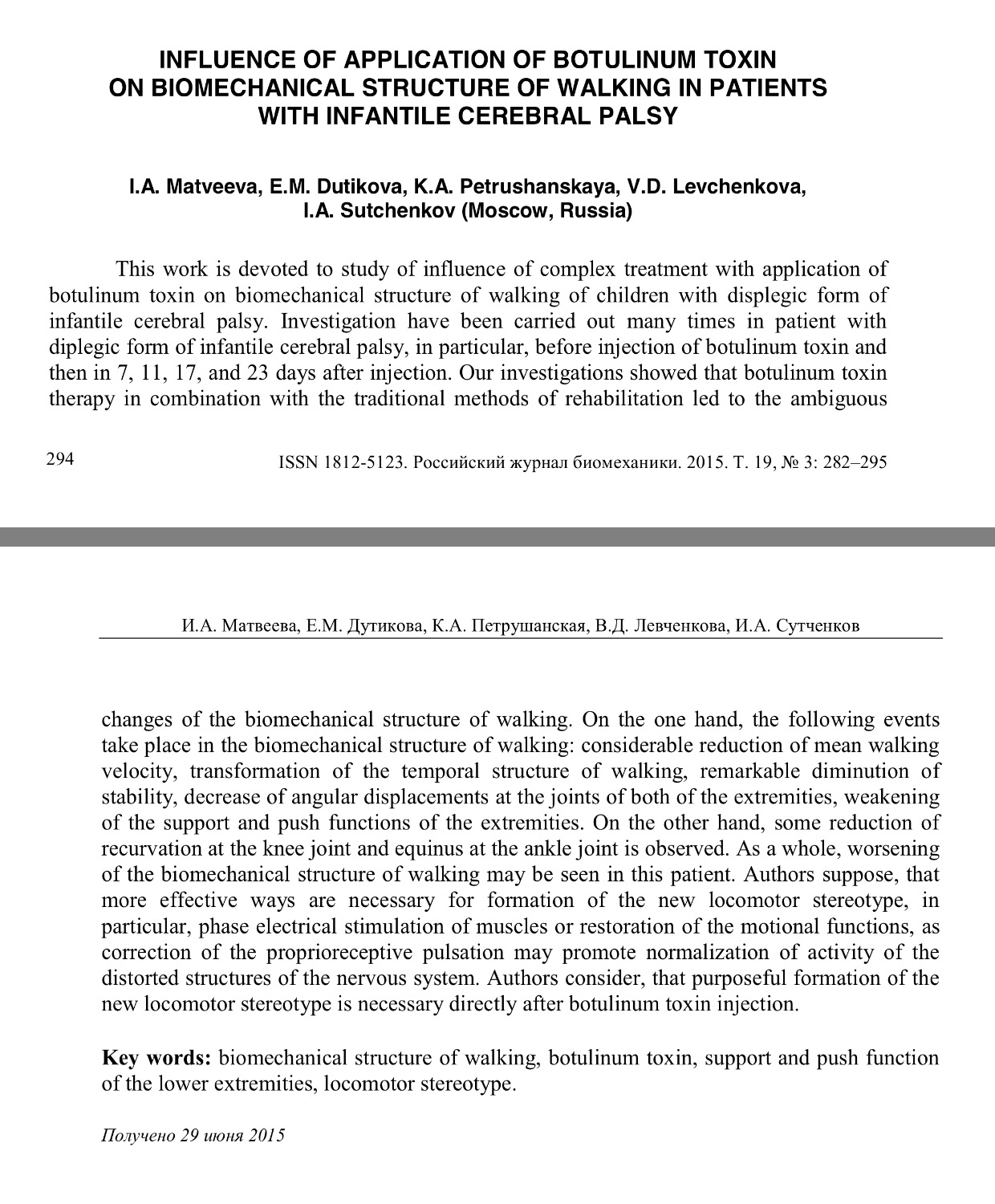
Last study I found about Botox: I advice you to read:
Mostly developed method fir CP but I am absolutely against (for walking child) I will not do for my son ….why?
Because it’s killing mussels and I give you some studies you must read about Botox:
Does the use of botox over long periods of time leads to decrease in its efficacy or atrophy of muscles?
I don’t know but I think that most clinicians will say that Botox will not prevent contractures but I’m not aware of any RCT type trial where patients have been followed long enough to establish if contractures developemnt is actually increased by Botox? But this is something that have been discussed, by clinicians as well as scientistc I would say . And feared by parents…I’m sure that you agree that other factors than spasticity cause contracture developemnt.
This is an old method that use to be used much more (in the 1970’s) and I had thought that it was largely abandoned with the availability of the baclofen pump and botox for specific muscle spasticity/spasms.
Because phenol damages the peripheral nerve, I decided to do a literature review to see if there are any recent studies on the subject, to see if there are any long term results….
Wong, et al. (2004) compared botox and phenol block on gait in children with cerebral palsy. They tested 27 ambulatory children with spastic cerebral palsy and found that the adverse effects of botox were less severe compared with phenol.
Most of the above studies are not randomized clinical trials. In 2002, van Kuijk, et al. did a literature search for randomized clinical trials (RCT) of neuronal and neuromuscular blockade, finding 4 RCTs for Botox and none for phenol. Although the evidence suggest that botox is safe, convincing evidence of efficacy was found only in two groups of patients: (1) patients with mild spasticity and a potential for voluntary extensor activity and (2) patients with severe spasticity suffering from problems of positioning.
Wolf & English (2000) studied the effects of peripheral nerve phenol block in rats and showed that it denervated muscle spindles (the sensors for muscle stretch) of both afferent (sensory) and gamma (motor control) fibers. After 6 weeks, most of the spindles (90%) showed return of the afferent fibers but only about a third (38%) showed return of gamma innervation.
I personally find this study interesting ( even if they found Botox good in short therm period)
It was interesting to read about ethyl alcohol and phenol .
As well as discussed mixture ethyl alcohol with ledocaine for dystonia ( and compared to injections for Wolff Parkinson’s wight syndrome by the way): but still we can have some adverse events like phlebitis….
As I mentioned before more than 2 years ago my friend from USA started an online closed support group on Facebook for HBOT called “HBOT for Pediatric Neurological Conditions”. She asked me to be the admin of the group and it so happened that she afterwards « gave » me the administration of this group. Now the group has become big ( more than 1800 members) of parents and professionals from the hbot feld.
And in fact this is our Hbot locations ( created in collaboration with parents and professionals present on Facebook page) if you want to contact directly referral parent of location or professional I invite you to become member of Facebook group and ask them questions directly.
We did Gyrostim and neurofeedback first time for Marc end of April 2017 in neuro plasticity brain center in France: ( one week) it’s like center in Orlando USA parents know what I talking about but in france and chiper (all therapies in USA I don’t know why but much more expensive in USA….)
In short : Vibramoov ™ uses Functional Proprioceptive Stimulations (SPF) to activate the nervous system with sensory information identical to that of natural walking.
These stimulations keep the sensory-motor interactions of anyone with locomotor disorders active and stimulate their neuroplasticity.
Experiments with vibramoov tests was developed by
Pr J-P Roll and now
by Prof. Frederic Albert, who was a student of Pr Roll
« Neurorehabilitation through Functional Proprioceptive Stimulations:
The Vibramoov system applies Functional Proprioceptive Stimulation to preserve the sensory and motor functions of the patient even when movement is impossible. A number of electromechanical actuators are placed as shown in the adjacent images. Programmed sequences stimulate the nervous system with sensory information which is identical to that which occurs in normal movement. This afferent information can induce motor responses corresponding to the sensation that the patient experiences. The patient has the sensation and experience of movement even at the earliest stage of recovery. It is safe and effective when applied early in rehabilitation.
Research findings suggest that the sensory feedback induced by Vibramoov and the associated perception of movement may counteract disuse-induced cortical plastic changes. This happens due to the recruitment of a large part of the cortical network which is normally used during the actual performance of a movement. This research supports the possibility of guiding cortical plasticity with proprioceptive augmented feedback.
Many acquired or congenital neurological impairments (such as stroke, incomplete spinal cord injury, traumatic brain injury, cerebral palsy, MS and Parkinson’s disease) can dramatically affect our ability to move at will and they disturb our sense of « connection » to and awareness of our limbs. Awareness of limb position (proprioception) is impaired.
One of the main challenges of neurorehabilitation is to preserve or re-establish the coordination between motricity (active movement) and the related neurosensory information.
Vibramoov offers a unique neurorehabilitation therapy by maintaining the functional interaction between movement and proprioception throughout the recovery process.
Vibramoov enhances both the rate and potential for recovery as the system may be used safely at the earliest stages of recovery; even earlier than typical robotic interventions.
Early intervention is very important to maximise the rate and extent of recovery as prolonged immobility brings about secondary effects that can be very hard to overcome when therapy is delayed. »
En août 2018 en plus des Gyrostim et autres programmes neroplasticity d’année dernière on a essayé nouvel système reheducation française Vibromoov!
Ce qui était intéressant, c’est que Marc faisant vibramoov aujourd’hui (sans bouger les jambes) avait des sentiments à marcher (je lui ai demandé ce qu’il ressentait et il a dit: je marche avec des petits pas) ….
Vibromoov est un nouveau système de rééducation innovant.
Centre que nous faisons Gyrostim est l’un des 4 centres en France à faire de la rééducation avec cet système.
En bref: Vibramoov ™ utilise des stimulations proprioceptives fonctionnelles (FPS) pour activer le système nerveux avec des informations sensorielles identiques à celles de la marche naturelle.
Ces stimulations maintiennent actives les interactions sensori-motrices de toute personne présentant des troubles locomoteurs et stimulent leur neuroplasticité.
Les expérimentations ayant procédés aux tests du vibramoov sont celles développées par le Pr J-P Roll et maintenant par le Pr Frederic Albert, qui a été étudiant du Pr Roll
« Technoconcept, lauréat du trophée Innovation et médecine.
Technoconcept : la révolution médicale mondiale
L’histoire de Technoconcept, c’est l’histoire d’une révolution médicale, baptisée « Vibramoov ». Après 30 ans de recherches scientifiques et cliniques, la société installée à Mane est parvenue à mettre au point une technologie révolutionnaire dans le monde de la rééducation. Le « Vibramoov » permet en effet, à partir de séquences de vibrations, de stimuler le système nerveux. Il s’agit, ni plus ni moins, d’envoyer au cerveau des informations liées au mouvement alors que le corps n’est pas en capacité de bouger !
« Sans stimulation, le cerveau oublie très vite et se met à dérailler », expliquent Frédéric Albert et Nicolas Plumier, respectivement manager R&D et manager marketing. « Plus le corps reste immobile longtemps, plus la rééducation est longue et difficile. Alors imaginez une personne victime d’un AVC, avant qu’elle puisse se remettre debout, des mois se seront écoulés Avec le Vibramoov, son cerveau n’aura jamais cessé de monter des escaliers ou de courir. On maintient les activités cérébrales et on peut agir très tôt dans le parcours de soins ».
Officiellement présenté en décembre dernier, le Vibramoov de Technoconcept débute sa phase de commercialisation. Et, comme l’on pouvait s’y attendre, l’accueil est à l’image du produit : exceptionnel. Des premières commandes ont déjà été enregistrées en France et les premiers centres seront équipés dans le courant du mois de juillet ; mais l’intérêt médical dépasse largement nos frontières… De l’Italie à l’Allemagne en passant par la Pologne, la République Tchèque ou le Royaume Uni, tous les plus grands spécialistes sont unanimes, certains professeurs n’hésitant pas à parler du « meilleur dispositif qu’ils aient vu dans toute leur carrière » !
Il faut dire que Technoconcept a également mis à profit les six derniers mois pour améliorer et optimiser les capacités du Vibramoov. Initialement programmé pour la rééducation des membres inférieurs, il peut désormais appliquer le même procédé pour les membres supérieurs afin de proposer une méthode globale de traitement. Sachant que personne d’autre n’est capable de faire ça … dans le monde entier !
La société Technoconcept a été créée en septembre 1998 ; installée dans la zone d’activité Pitaugier, à Mane, elle emploie 16 personnes et est cogérée par Daniel Boschat, Frédéric Albert et Nicolas Plumier. »
I found this center like in Orlando USA ( but cheaper and in France)😉I honestly think they may be have more therapies also for neurological plasticity to chèque hire:
In 1997 GyroStim inventor Kevin Maher and his wife gave birth to a little girl. Unfortunately, she was born three months premature, resulting in a diagnosis of severe spastic quadriplegia cerebral palsy. When she reached age 4, her parents were told that her very poor balance might benefit from including vestibular stimulation in her daily home therapy program. She was prescribed a regimen of hundreds of chair spins, log rolls, and somersaults every day. This additional therapy was back-breaking work, balance, and there was no comfortable, practical, or easy method to provide it. There had to be a better way.
Inspired by this problem, Kevin applied his 25 years of experience with robotics systems towards engineering a solution. He designed and built an easier, safer, and more efficient way to provide his daughter with vestibular stimulation, resulting in the first prototype of the GyroStim. Maher’s daughter, Mackenzie, made unexpected and rapid gains, not only in balance, but also in other gross and fine motor abilities, trunk control, energy level, speech, and overall abilities. It soon became apparent that the vestibular stimulation from his unique combination of pitch and yaw rotations had triggered a cascade of significant additional gains well beyond the goal of simply improving her balance.
The Launch
Kevin continued developing his unique rotating chair, and soon his work captured the attention and interest of therapists, doctors, and researchers. Their acknowledgment of the immense need for this innovative device and his desire to make it available to others who could benefit from it reinforced his decision for moving forward with development of the GyroStim and the launch of a new company, UltraThera Technologies.
Soon after the company was formed, the first GyroStim system sale was to the United States Air Force Academy. The second sale went to the Mayo Clinic Aerospace Medical Vestibular Laboratory, further validating the broader interest in his new technology, with additional sales soon to follow.
The Breakthrough
In January 2011, one of the NHL’s top athletes, Sidney Crosby, suffered back-to-back concussions that forced him out of the game for most of that year. As recovery continued to elude Crosby, many feared that the head injury would force him out of the game permanently just as his career was at its peak.
In August 2011, still suffering from debilitating post-concussion symptoms (PCS), it was recommended to Crosby that he try the GyroStim. Soon after, he was back on the ice and was eventually cleared for full contact practice. In November 2011, after nearly 11 months of being sidelined due to the concussions, Sidney Crosby returned to the ice in one of the most spectacular comeback games in history. In 2012, he went on to sign a 12-year $104.4M contract extension with the Pittsburg Penguins, and GyroStim went on to become widely recognized for being the breakthrough technology that helped Crosby overcome his concussions.
The Paradigm Shift: From Passive to Interactive
Through 2013, GyroStim was used to provide passive vestibular stimulation— meaning that the subject seated in the rotating chair received vestibular stimulation without challenges or interactions during rotation. While this simple application of GyroStim was beneficial in many cases, Maher believed passive stimulation was only the beginning of what could be accomplished using GyroStim.
Maher hypothesized that adding an interactive training element during the vestibular stimulation would engage, challenge, and improve the function of physical and cognitive systems (sensorimotor systems) activated during the exercise. Theoretically, this would improve not only balance but also improve the performance of the activated sensorimotor systems, resulting in improved cognition and overall human performance.
To explore this hypothesis, he developed an integrated laser targeting system to provide subjects with interactive challenge during rotation. The subject would use a laser pointer to hit as many targets as possible—while rotating in the GyroStim. This interactive “perceive, process, and react » approach should present significantly greater challenge to the subject’s physical and cognitive abilities than simply receiving passive vestibular stimulation in the GyroStim.
Maher also developed a library of motion profiles, with each profile providing a specific level of intensity, ranging from Level 1 (lowest intensity) to Level 30 (highest intensity). This would allow the clinician to quickly select a level and present the subject with vestibular stimulation and sensorimotor exercises advancing at an appropriate pace for each individual as performance improved. In other words, the GyroStim system and method customize an optimized rate of advancement for each person based entirely on their own performance progress.
In 2014, Maher put his interactive approach to the test during training camps with NFL, NHL, professional boxing/MMA, and Olympic athletes. The positive outcomes achieved supported his hypothesis with nearly all athletes reporting significant improvements in the areas of balance, coordination, spatial and situational awareness, reaction time, hand-eye coordination, object tracking, reduced brain fog, improved sleep, and also better mood, faster reading speed and improved comprehension were reported.
From there, Maher surmised that this same interactive approach for improving athletic performance would also be beneficial when used at lower intensities to help individuals during the rehabilitation and recovery process. His theory was supported by the reports of clinicians and thousands of people from all walks of life who have benefitted from using GyroStim at lower levels of intensity.
This method of applying vestibular stimulation and sensorimotor exercises simultaneously while incrementally advancing the intensity of training has transformed and greatly expanded applications for GyroStim on both ends of the spectrum from injury and illness rehabilitation to athletic performance enhancement.” ( Source: http://www.gyrostim.com/evolution.html )
Oxygen could be toxic if not administered properly, so that’s why I want tell parents about this fact and I advice to take consultation with specialist ( of your choice) before any HBOT treatment ( whichever type of pressure or type of chambers you choose to use it’s safer if treatment monitored by HBOT doctor especially if supplemental oxygen is added)
Part I
Oxygen toxicity:
Protocols for the avoidance of hyperoxia exist in fields where oxygen is breathed at higher-than-normal partial pressures but protocol must be monitored.
But not much centers are doing complete check up ( as i am doing for Marc before/after HBOT)
EKG
Blood tests
Medical tests and checking his tubes and ears
Vision tests
His heart beats / pulse rate and pressure and oxymeter are measured, every day before/and after HBOT
So I know that he doesn’t get oxygen toxicity from his HBOT treatment.
Patients at risk for pulmonary oxygen toxicity should be monitored for oxygen saturation and increased work of breathing. They can be evaluated by pulmonary function testing and chest x-rays which can show signs of ARDS.
(In Israel we did X-Rays for marc and me(as we are going with him inside the chamber)
Similarly, eye exams assessing acuity and looking for lens opacification can be done to detect early ocular oxygen toxicity. (Also did all ayes tests before starting HBOT)
CNS toxicity manifests as described and will often have tachycardia and diaphoresis as well. (as well because my son condition is WPW = tachycardia possible in his case so this point and blood pressure is monitored every day)
Aborting a hyperbaric exposure when these signs are present can prevent seizure occurrence!!
So here or file with docs to read:
Oxygen Toxicity :
The effects of oxygen toxicity may be classified by the organs affected, producing three principal forms:
• Central nervous system, characterised by convulsions followed by unconsciousness, occurring under hyperbaric conditions;
• Pulmonary (lungs), characterised by difficulty in breathing and pain within the chest, occurring when breathing increased pressures of oxygen for extended periods;
• Ocular (retinopathic conditions), characterised by alterations to the eyes, occurring when breathing increased pressures of oxygen for extended periods.
Central nervous system oxygen toxicity can cause seizures, brief periods of rigidity followed by convulsions and unconsciousness, and is of concern to divers who encounter greater than atmospheric pressures. Pulmonary oxygen toxicity results in damage to the lungs, causing pain and difficulty in breathing. Oxidative damage to the eye may lead to myopia or partial detachment of the retina. Pulmonary and ocular damage are most likely to occur when supplemental oxygen is administered as part of a treatment, particularly to newborn infants, but are also a concern during hyperbaric oxygen therapy.
Oxygen toxicity seizures (Bert effect) can occur with hyperbaric oxygen therapy in a dose-dependent relationship. The overall risk may be as frequent as 1 in 2000 to 3000 treatments. However, this risk may be as high as 1 in 200 at higher pressures (2.8 to 3.0 times normal atmospheric pressure or one atmosphere absolute (ATA)) and as low as 1 in 10,000 for treatment at 2 ATA or less. One study looking at the hyperbaric treatment of decompression illnesses noted an overall incidence of oxygen toxicity events of 7%. The incidence of pulmonary toxicity (Smith effect) was 5%, while 2% for central nervous system symptoms, and a seizure rate of 0.6%.
Central nervous system signs and symptoms:
• Headache
• Irritability and anxiety
• Dizziness
• Disorientation
• Hyperventilation
• Hiccups
• Cold shivering
• Fatigue and restless ( difficulty to sleep)
• Tingling in the limbs
• Visual changes such as blurring and tunnel vision
• Tinnitus and Hearing disturbances
• Nausea
• Twitching
• Tonic–clonic seizure
Pulmonary toxicity signs and symptoms:
• Mild tickle sensation on inhalation
• Mild burning on inhalation
• Uncontrollable coughing
• Hemoptysis
• Dyspnea
• Rales
• Fever
• Hyperemia of the nasal mucosa
• CXR shows inflammation and pulmonary edema
Eyes:
• In premature babies, retinopathy of prematurity and retrolental fibroplasia
• Cataract formation (long-term exposure)
And now some studies about and links:
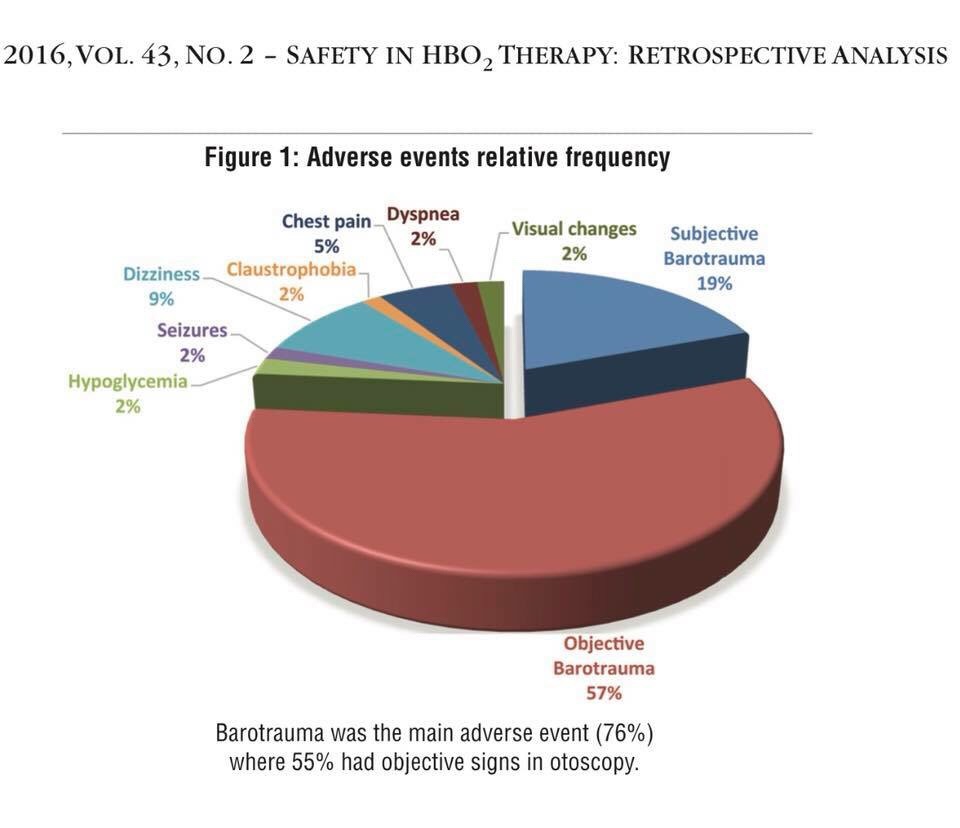
1) Several side effects and complications from hyperbaric oxygen (HBO2) therapy have been described, with varying degrees of seriousness. By far, the two most frequent and benign side effects comprise middle ear barotrauma, which has been noted in up to 2% of treated patients, and can be prevented or minimized by teaching autoinflation techniques, or by inserting tympanostomy tubes. Another frequent complaint is claustrophobia, both during multiplace and monoplace chamber compression, requiring reassurance, coaching and, at times, sedation. Other more rare, but more severe side effects derive from oxygen (O2) toxicity, from the multiple exposures required for chronic treatments, especially progressive myopia, usually transient and reversible after stopping HBO2 sessions, or pulmonary dyspnea, with cough and inspiratory pain. More serious O2-induced seizures happen rarely, at higher O2 pressures, and often during acute treatments in acidotic patients (carbon monoxide poisoning). Source :
2)Oxygen delivered in supraphysiological amounts is currently under investigation as a therapy for brain injury. Hyperoxia can be delivered to the brain under normobaric as well as hyperbaric conditions. In this study the authors directly compare hyperbaric oxygen (HBO2) and normobaric hyperoxia (NBH) treatment effects.
And here if somebody wants to read comparaison bethween normobaric and hyperbaric oxygen toxicity :
( oh it’s TBI but the same processes we have for all human metabolism for others injuries as well….)
« Hyperbaric O2 has a more robust posttreatment effect than NBH on oxidative cerebral metabolism related to its ability to produce a brain tissue PO2 ≥ 200 mm Hg. However, it appears that O2 treatment for severe TBI is not an all or nothing phenomenon but represents a graduated effect. No signs of pulmonary or cerebral O2 toxicity were present. »
Under normobaric conditions, the majority of oxygen is transported within the erythrocytes bound to hemoglobin. Breathing of 100% oxygen already results in a 100% saturation of hemoglobin.
5)Dr. J. Lorrain Smith first described the toxic effect of oxygen on the lungs in 1899. He noted that the severity of the effect increased with increasing pO2 and that the effects where largely reversible. As shown in the diagram, the toxic effects of oxygen at partial pressures between 0.45 ATA and 1.6 ATA are primarily on the lungs while the toxic effect at pO2s over 1.6 ATA are primarily on the brain.
The earliest sign of pulmonary (lung) oxygen toxicity is a mild irritation in the trachea (throat) that is made worse with deep inspiration. A mild cough develops next, followed by more severe irritation and cough until inspiration becomes quite painful and the cough becomes uncontrollable. If exposure to oxygen is continued, the person will notice chest tightness, difficulty breathing, shortness of breath, and if exposure is continued long enough, the person will die, from lack of oxygen! The progressive damage to the lungs eventually makes it impossible for the oxygen to get to the blood as it passes through the lungs. The time to onset of symptoms is highly variable but most individuals can tolerate 12-16 hours of oxygen at 1.0 ATA, 8-14 hours at 1.5 ATA, and 3-6 hours at 2.0 ATA before developing mild symptoms. There are several ways to track developing pulmonary oxygen toxicity but the most sensitive and accurate is the development of symptoms. A second technique is to monitor the vital capacity. Vital capacity (the amount of air that can be moved in one large breath) decreases with increasing pulmonary toxicity. A reduction of approximately 2% in vital capacity correlates with mild symptoms while a reduction of 10% correlates symptoms so severe that most individuals will not voluntarily continue breathing oxygen. These mild effects are completely reversible and no permanent lung damage occurs. However, the damage will take 2 to 4 weeks to heal. The pathology of pulmonary oxygen toxicity is understood but beyond the scope of this discussion.
A third way to keep track, in rough terms, of pulmonary oxygen toxicity is to keep track of the oxygen exposure. This technique is called calculating the Unit Pulmonary Toxic Dose (UPTD) and one UPTD is equivalent to breathing 100% oxygen, for one minute, at 1.0 ATA. As a guide, 615 UPTDs in one day will cause a 2% reduction in vital capacity and 1,425 units will cause a 10% decrease. There are several different ways to calculate the UPTD (some try to correct for increasing toxic effects with increasing dose, in addition to the simple pO2) and there is quite wide variation in individual tolerance so that symptoms are still the best guide. The situation where UPTDs are most useful is in planning a large number of dives, in a few days, all involving a large amount of oxygen decompression or CCR diving. Even then, the dive plan may have to be altered if the diver develops symptoms of pulmonary toxicity.
The first and most important method to prevent pulmonary oxygen toxicity is to limit exposure to the lowest possible pO2 for the shortest period of time.
The second method to prevent pulmonary oxygen toxicity is to provide air breaks.







 very good marketing 👏 bravo
very good marketing 👏 bravo