Le 27 mars 2018 nous sommes partis pour Sofia, en Bulgarie, afin de récupérer un PONS Device. Notre fils a entamé une rééducation par ce biais dès le lendemain. Mais laissez-moi vous expliquer comment j’ai eu connaissance de cette technologie en premier lieu.
J’avais lu le livre de Norman Doidge, ouvrage conseillé par d’autres parents d’enfants cérébrolésés. Heureusement, sur Facebook se trouvent beaucoup de groupes privés, qui permettent à certaines personnes, intéressées par un même sujet, d’échanger à volonté.
C’est de cette manière que j’ai pris connaissance de l’existence du chercheur Youri Danilov, qui pilotait une étude clinique sur la technologie PONS. Je lui ai envoyé un message dans l’instant suivant et j’ai eu la chance qu’il me réponde. Nous avons ensuite conversé par Skype, et il a confirmé que cela pourrait aider Marc d’essayer, même si l’étude clinique était en cours et que les résultats n’étaient pas encore validés. Il faut savoir que le processus est extrêmement long avant d’obtenir une validation par les instances de santé correspondantes.
Un des avantages non négligeables de la technologie PONS était qu’elle ne présentait absolument aucun risque. Elle n’était pas non plus invasive. Marc n’avait absolument rien à perdre. Mais il fallait récupérer l’appareil sur place pour engager la location et faire une formation auprès de professionnels de santé afin de s’entraîner à manipuler l’appareil correctement.
Il était possible de récupérer un PONS Device en location, en Russie ou en Bulgarie. Pour des questions d’obtention de visa, il était plus rapide de s’orienter vers la Bulgarie, et c’est donc vers ce pays que nous nous sommes envolés.
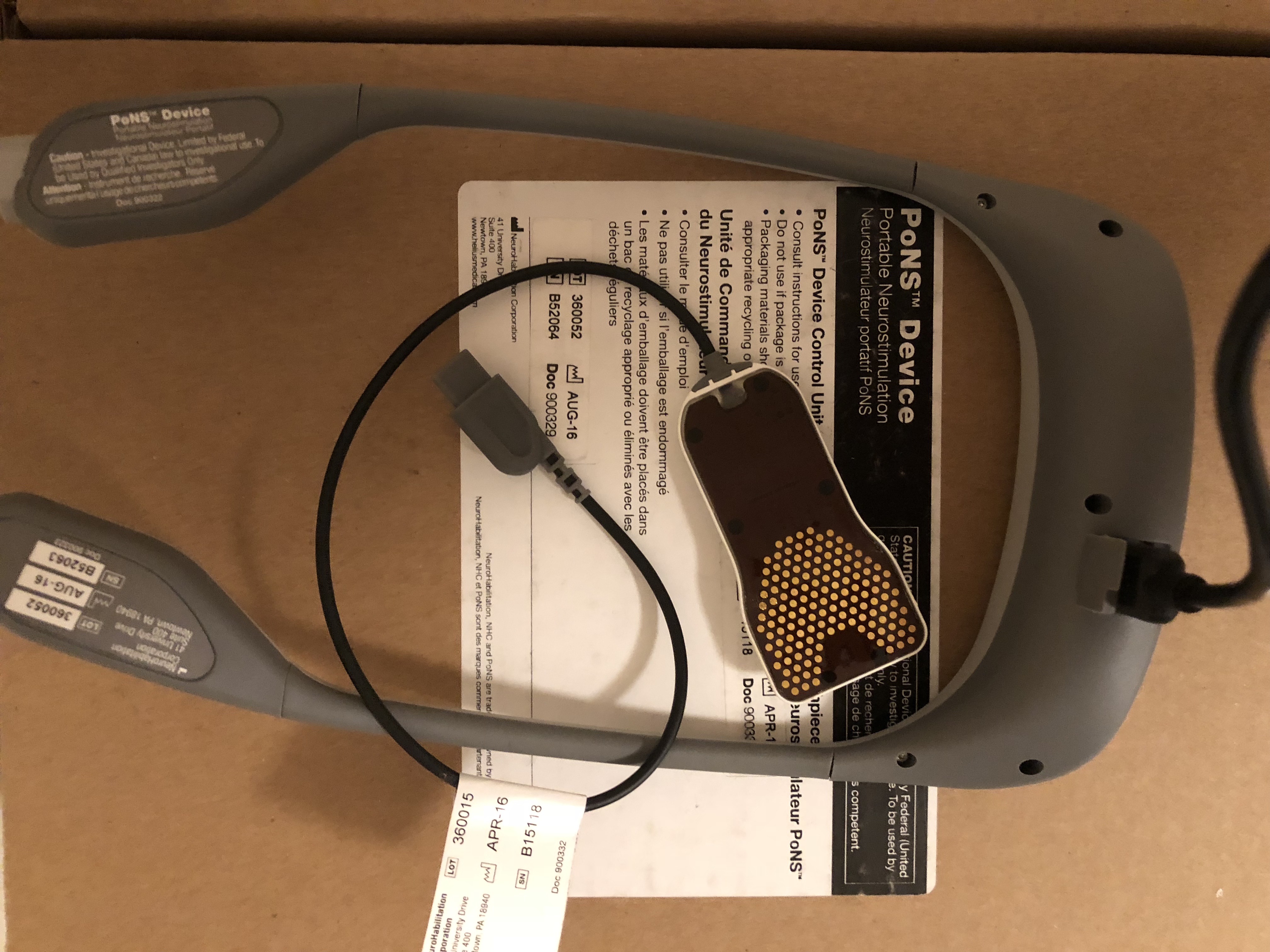
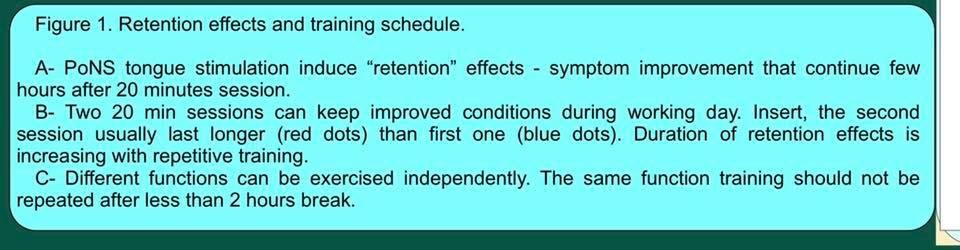
Comment l’appareil PONS fonctionne-t-il ? Par électrostimulation, par l’intermédiaire de cent quarante-trois petites électrodes positionnées sur une languette. Cette languette doit être coincée sous la langue, dont le seuil d’excitabilité est extrêmement faible. Les impulsions rallient le cerveau très rapidement sans aucune douleur, dans une zone très spécifique. Au début, la puissance est réglée à son niveau le plus bas, puis l’intensité peut être augmentée progressivement, selon les progrès du patient.
En 2018, cette technologie a reçu l’autorisation de mise sur le marché au Canada et elle est utilisée légalement depuis, en dehors des études cliniques. Mais son coût est prohibitif : trente mille dollars canadiens pour quatorze semaines de location ! Or, les chercheurs qui se sont impliqués dans les recherches initiales pensaient que l’idée était de faire rembourser l’appareil par le gouvernement, pas de mettre les patients à sec financièrement ! D’autant que, par l’expérience de Marc, je peux affirmer que quatorze semaines ne sont pas suffisantes pour que les progrès d’un patient soient durables… Mon fils a commencé à utiliser l’appareil fin mars 2018, nous en sommes donc à plus d’un an d’utilisation, avec une pause lorsque le fil du chargeur s’est abîmé et qu’il ne remplissait plus son office.
Par ailleurs, j’ai dû me procurer plusieurs languettes d’avance, car celles-ci sont programmées et elles arrêtent de fonctionner au bout de trois mois. Elles ne peuvent pas être ré-encodées en l’état, il faut donc en changer régulièrement. Et je ne vais pas retourner en Bulgarie ou en Russie tous les trois mois.
Le 30 mars, nous avons enchaîné sur le trajet Bulgarie-Israël. Au programme, une autre série de séances hyperbares : trente heures à réaliser entre le 2 avril et le 12 mai. Donc nos résultats c’est un mélange cet fois- ci de pons + hyperbare.
Au bout de trois ou quatre semaines, nous avons commencé à constater les effets du PONS Device et des séances hyperbares. Marc est devenu plus habile.
Donc résultats Pons+ Hbot:
Le 12 mai, nous sommes revenus à Grenoble. Marc a repris l’école à ce moment-là. Le personnel du groupe scolaire n’en revenait pas ! Tous disaient l’avoir vu renaître… À la maison, nous avons eu la surprise de voir Marc commencer à manipuler des petits Legos, là où, auparavant, il n’utilisait que des gros blocs (style Duplo®). Quel progrès !
Fin juillet 2018, Marc a commencé à s’habiller tout seul. Là, j’attribue au PONS son amélioration en motricité fine : de même que Marc pouvait alors manipuler les Legos de son âge, il pouvait aussi attraper ses vêtements avec plus de dextérité.
Le 31 décembre 2018 l’appareil PONS est tombé en panne : une faiblesse au niveau du chargeur. Le temps de demander des visas pour la Russie (le centre bulgare ne gérait plus les PONS) et, en février 2019, nous sommes partis dans mon pays natal pour la réparation. Finalement, la prise du chargeur n’a pas pu être réparée, nous avons dû carrément changer l’appareil en location.
Nous sommes restés sur place quinze jours pour de la rééducation accompagnée dans le centre médical. Le kiné sur place ne parlait que le russe, mais il a su nouer une communication avec Marc et les séances se sont déroulées sans souci. C’est avec lui que Marc a monté pour la première fois à nouveau quelques marches d’escalier, sans se tenir du tout ! Ce kiné a aussi inventé une planche d’équilibre soutenue par 2 ballons, placés de part et d’autre. Cela sert à améliorer l’équilibre avant/arrière ou droite/gauche des patients. Ils peuvent ainsi travailler une compétence à la fois.
De Russie, j’ai ramené un DENAS, un autre appareil de neurostimulation transcutanée, utilisé cette fois en vue d’apaiser la douleur.
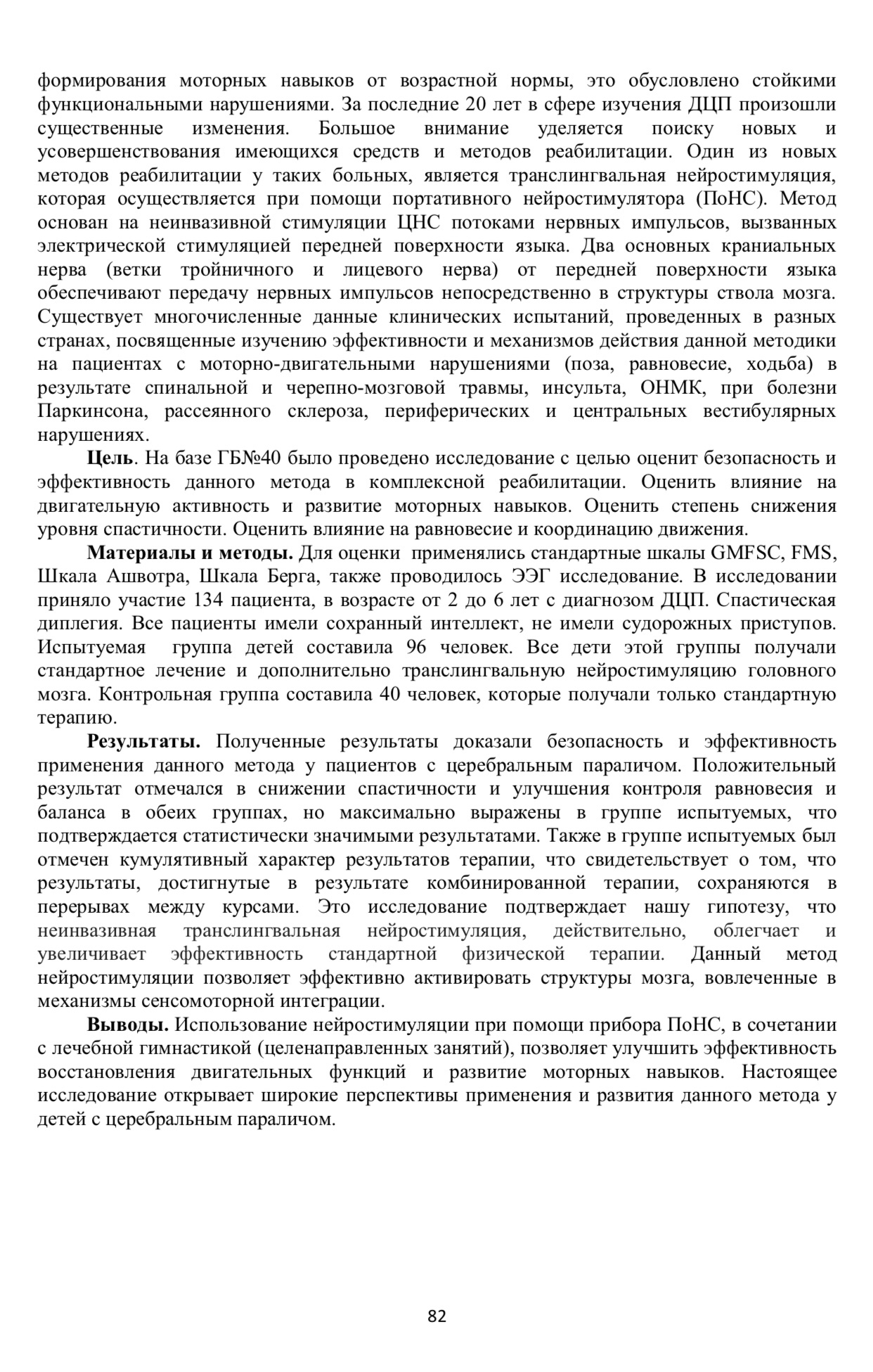
Scientific part ( studies):
2003,
First discovery of retention effects after tongue stimulation
Tyler, M., Danilov Y.P., Bach-y-Rita, P. Closing an open-loop control system: vestibular substitution through the tongue. J. Integr. Neurosci. 2, 2, 2003
2004,
First description of multiple positive effects of tongue stimulation
Yuri Danilov. Vestibular substitution for posture control, In.: Innovations technologiques et Handicap, Actes des Entretiens de l’Institut Garches, eds: F. Lofaso, JF Ravaud et A. Roby-Brami, Frison-Roche, Paris, 2004, pp. 216-225
2005,
Summary and perspective vision of use tongue stimulation in rehabilitation
Bach-y-Rita P, Danilov YP, Tyler ME, Grimm RJ. Late Human Brain Plasticity: Vestibular Substitution with a Tongue BrainPort Human-Machine Interface. J Intellectica. 2005, 40, pp. 115-122.
First two TBI patients demonstrate remarkable improvement after 2 weeks of training, at Chateau Rauzé Rehabilitation centre (specialized exclusively in the treatment of TBI) at Cénac near Bordeaux France._
PET scan study demonstrate rearrangement of brain activity after tongue stimulation in blind subjects
Ptito, Maurice, et al. « Cross-modal plasticity revealed by electrotactile stimulation of the tongue in the congenitally blind. » Brain 128.3 (2005): 606-614._
2007,
First 28 patients with vestibular loss.
Danilov Y. P., Skinner K. L., Tyler M. E., Bach-y-Rita P. Efficacy of electrotactile vestibular substitution in patients with bilateral vestibular and central balance loss, JOVR, 2007, 17, 119-130
2008
Independent verification in France, 8 vestibular los patients
Nicolas Vuillerme , Nicolas Pinsault, Olivier Chenua, Jacques Demongeota, Yohan Payan , Yuri Danilov. Sensory supplementation system based on electrotactile tongue biofeedback of head position for balance control, Neuroscience Letters, 431, 3 (2008) 206-10
2009
The first textbook chapter about vestibular substitution
Danilov, Y. P., Tyler, M. E. and Kaczmarek, K. A. (2008). Vestibular sensory substitution using tongue electrotactile display. In Human Haptic Perception: Basics and Applications (Grunwald, M., Ed.), Birkhauser Verlag, Basel, Switzerland. (invited review), Chapter 39, pp. 467-480
2010
First independent objective verification of tongue stimulation effects using fMRI
Wildenberg, J.C., Tyler, M.E., Danilov, Y.P., Kaczmarek, K.A., Meyerand, M.E. (2010) Sustained cortical and subcortical neuromodulation induced by electrical tongue stimulation. Brain Imaging and Behavior.
Independent verification in Brasil
Barros, C.G., Bittar, R.S., Danilov Y. Effects of electrotactile vestibular substitution on rehabilitation of patients with bilateral vestibular loss, Neuroscience Letters, 476, 3 (2010) 123-6
2011
UW-Madison, fMRI verification continued
Joseph C. Wildenberg, Mitchell E. Tyler, Yuri P. Danilov, Kurt A. Kaczmarek, Mary E. Meyerand. Electrical tongue stimulation normalizes activity within the motion-sensitive brain network in balance-impaired subjects as revealed by group-ICA. (2011). Brain Connectivity.
Joseph C. Wildenberg, Mitchell E. Tyler, Yuri P. Danilov, Kurt A. Kaczmarek, Mary E. Meyerand. High-resolution fMRI detects neuromodulation of individual brainstem nuclei by electrical tongue stimulation in balance-impaired individuals (2011). Neuroimage 56, pp. 2129-2137
Joe C. Wildenberg, Mitchell E. Tyler, Yuri P. Danilov, Kurt A. Kaczmarek, and Mary E. Meyerand. Altered Connectivity of the Balance Processing Network After Tongue Stimulation in Balance-Impaired Individuals. Brain Connectivity, 3,1, ( 2013), 87-97.
First use of tongue stimulation for stroke patients
Badke MB, Sherman J, Boyne P, Page S,Dunning K. Tongue-based biofeedback for balance in stroke:results of an 8-week pilot study. Arch Phys Med Rehabil 2011;92:1364-70.
2014
First controlled study with MS patients, , UW-Madison
Tyler, ME, Kaczmarek, KA, Rust KL, Subbotin AM, Skinner, KL, Danilov, YP. (2014) Non-invasive neuromodulation to improve gait in chronic multiple sclerosis: a randomized double blind controlled pilot trial. Journal of NeuroEngineering and Rehabilitation, 11:79.
Feasibility study on spinal cord injury subjects (SCI), Canada
Chisholm, Amanda E., et al. « Feasibility of sensory tongue stimulation combined with task-specific therapy in people with spinal cord injury: a case study. » Journal