As I promised, I am publishing a full report after our trip to Uzbekistan (Tashkent):
First of all, why did we go there? I already knew Dr. Bugorsky before, we visited him in a clinic near Moscow in 2019, you can read about it on my blog: https://brain-injury-hope.com/2019/02/pons-2-clinic-near-moscow/
But now traveling to Russia for treatment from abroad is not realistic! Therefore, naturally, when I found out that he opened a clinic in Uzbekistan and that you can buy a new Rehaline machine there instead of PoNS, we flew to Tashkent. And besides, I wanted to try spinal stimulation:
The invention of spinal stimulation belongs to Gerasimenko and the patent is also Russian and USA / and he personally advised me to go to Evgeniy in Uzbekistan…(yes, I correspond by email with dr Gerasimenko).
Well, first of all: Tashkent is a very beautiful modern city and Uzbekistan is completely open for visiting by foreign tourists (it’s a very safe city; I was at the French embassy about this and discussed the security situation – for 3 years there has not been a single case of robbery of French tourists!)
In Paris there are more problems with robbing Uzbek students than with tourists in Tashkent! But the flight time to Tashkent by plane is very long: 6 hours of flight from Paris and back 7 hours and 30 minutes! Of course it’s too far!
A lot of countries do not need a visa (Europeans/USA, Australia, etc.)…90 countries have the possibility of visa-free entry into Uzbekistan.
But the negative: firstly, this is a former post-Soviet republic (quite poor population), the clinic has not yet organized a special meeting at the airport for foreigners, and local taxi drivers who will literally “attack” you when leaving the airport, persistently trying to sell you a taxi – may shock you a little 😜 actually, their service for disabled people in Tashkent is poorly established (until the clinic improves it – traveling with a child in a wheelchair is very difficult – there are a lot of stairs / there are no elevators!)
The second negative: almost no one speaks English (a translator is definitely needed – but again, this service has not yet been established at the clinic, but they said it will be established)…. But everyone speaks Russian – yes, parents like me,
from the former Soviet- union will be quite familiar with situation.
Positive:
Very tasty and inexpensive food: “PLOV”! (so many types!) Did you know that in December 2016, “PLOV” was added to UNESCO’s list of intangible heritage? Now you know!
meat: how do they cook veal & beef and lamb like this? I don’t know, but it’s very tasty – and very cheap (compared to the USA, everything is natural / gorgeous local fruits / awesome local cuisine – very similar to Turkish but with seasonings and be sure to ask if it’s spicy 🌶️….
In addition to PLOV and lagman, national Uzbek cuisine is proud of such dishes as basma (meat stewed with vegetables), manti (finely chopped meat rolled into thin dough; the dish is steamed), chuchvara (dumplings), shurpa (soup with meat and potatoes ).
So far, 2 floors of the clinic are completely ready (separate rooms for accommodation with shower and toilet), accommodation in the clinic itself is very cheap compared to a hotel per night… (but honestly, I personally don’t like being accommodated in a clinic and generally living in hospital conditions, although the clinic and rooms are European level) but personally we don’t like living in hospitals… and a hospital environment when you go out into the corridor and there are other patients there, etc….
Therefore, we always prefer to live and asked to study in our 4* hotel, especially since it was the New Year holidays and the clinic was closed on New Year’s Day! Yes, that’s why both the doctor Dr. Bugorsky and the physical therapist came to our hotel! I discussed this with the doctor in advance because we could only come during the New Year…
But naturally, we personally saw the clinic and 2 floors have been completely completed – the clinic will be even larger since the remaining 3 floors will also be completed and the cosmetology direction will also be open and possible (the use of exosomes both for cosmetology and for the treatment of cerebral palsy and Autism) they are in the process negotiations with the center in Samara (from where I received exosomes for Mark)…. But these are plans and how it turns out… we’ll see…
And the last video interview with dr Bugorsky (where I ask questions that parents of children with cerebral palsy asked me) which I already published to you before:
Как я и обещала я публикую полный отчет после нашего путешествия в Узбекистан ( Ташкент):
Во первых почему и туда поехали? Я уже до этого знала dr Bugorsky мы были у него в клинике рядом с Москвой в 2019 году вы можете почитать об этом на моем блоге :
Pons 2 ( clinic near Moscow) – Brain Injury Hope
Но теперь ездить в Россию на лечение из за границы- не реально ! Поэтому естественно когда я узнала что он открыл клинику в Узбекистане и что можно там приобрести новую машину Rehaline вместо PoNS мы полетели в Ташкент. И кроме того я хотела попробовать спинальную стимуляцию :
Изобретение спинальной стимуляции принадлежит Gerasimenko и патент так же русский и США / и он мне лично посоветовал ехать к Евгению в Узбекистан …( да я переписываюсь по майлу с dr Gerasimenko) .
Ну во первых : Ташкент очень красивый современный город и Узбекистан открыт полностью для посещения иностранными туристами ( очень безопасный город я по этому поводу была во французском посольстве и обсуждала ситуацию о безопасности – за 3 года ни одного случая ограбления французских туристов! )
В Париже больше проблем с ограблением узбекских студентов чем с туристами в Ташкенте! Но время полета до Ташкента в самолете – очень длинное 6 часов полета из Парижа и обратно 7ч30 минут! Конечно далековато!
Виза не нужна очень многим странам ( европейцам/ из USA из Австралии и т д)…90 стран имеют возможность безвизового въезда в Узбекистан .
Но негатив : во – первых это бывшая пост советская республика ( достаточно бедное население) пока не организована еще клиникой спец- встреча в аэропорту для иностранцев а местные таксисты которые будут вас в буквальном смысле « атаковать» при выходе из аэропорта настойчиво пытаясь продать вам такси – может вас немного шокировать 😜 вообще-то у них сервис для инвалидов в ташкенте плохо налажен ( пока клиника не наладит – ехать с ребенком на инвалидном кресле – очень тяжело – много лестниц / не предусмотрены лифты!)
Второй негатив: практически никто не говорит по английски ( обязательно нужен переводчик – но опять же этот сервис еще не налажен у клиники но будет налажен они сказали)…. Зато все говорят по русски – да родителям как я,
из бывшего союза будет достаточно привычно и легко разобраться .
Позитив:
Очень вкусная и не дорого еда : “PLOV”! ( столько типов!) Did you know that in December 2016, “PLOV” was added to UNESCO’s list of intangible heritage? Now you know!
мясо : как они так готовят телятину & говядину и баранину ? Не знаю но очень вкусно – и очень дешево ( по сравнению с сша все натуральное / шикарные местные фрукты / обалденная местная кухня – очень похожая на турецкую но с приправами и обязательно спрашивайте если spicy 🌶️….
Помимо плова и лагмана национальная узбекская кухня гордится такими блюдами, как басма (мясо, тушенное с овощами), манты (мелко рубленное мясо, закатанное в тонкое тесто; блюдо готовится на пару), чучвара (пельмени), шурпа (суп с мясом и картофелем).
Пока готово 2 этажа клиники полностью ( отдельные комнаты для размещения с душем и туалетом) очень дешевое по сравнению с отелем размещение в самой клинике за ночь … ( но честно мне лично не подходит размещени в клинике и вообще жить в больничных устовиях хотя клиника и комнаты европейского уровня ) но лично мы не любим жить в больницах … и больничном окружении когда выходишь в коридор а там другие больные и тд ….
Поэтому мы предпочитаем всегда жить и попросили заниматься в нашем 4* отеле тем более ( что были новогодние праздники и на Новый год клиника закрыта) ! Да поэтому к нам и врач dr Bugorsky и кинетерапевт приходили в отель ! Я это заранее обговорила с врачем потому как приехать мы могли только в период нового года …
Но естественно мы лично видели клинику и там полностью доделаны 2 этажа – клиника будет еще больше так как оставшиеся 3 этажа тоже будут сделаны и так же будет косметологические направление открыто и возможно ( применение экзосом и для косметологии и для лечения ДЦП и Аутизма) они в процессе переговоров с центром в Самаре ( откуда я получила экзосомы для Марка) …. Но это планы а как получится … посмотрим ….
И последние видео интервью с dr Bugorsky ( где я задаю вопросы которые мне задавали родители детей с дцп ) которое я уже вам до этого публиковала:
L’association Ma Rééducation Collective (MARC) est née de la volonté de Mme SERIGNY de donner aux enfants souffrants de paralysie cérébrale, comme son fils unique Marc, les outils techniques et scientifiques leur permettant de réussir au mieux leur rééducation.
Celle-ci est essentielle à ces enfants cérébro lésés afin qu’ils puissent gagner suffisamment d’autonomie pour être indépendant à l’âge adulte.
Elle a constaté qu’il y a une demande importante pour des stages intensifs en voyant tous les parents partirent à l’étranger là où des offres existent.
Cette association a pour objectifs de :
⦁ Soutenir la rééducation d’enfants atteints de paralysie cérébrale de niveau GMFCS ( Gross Motor Function Classification System * ) niveau 1 et 2 , freinés dans leurs apprentissages de la motricité et dans leur développement.
⦁ Partager l’expérience, les connaissances théoriques des différentes therapies et nouveautés technologiques qui se développent au niveau mondial pour les enfants atteints de paralysie cérébrales
⦁ Promouvoir les solutions ayant fait leurs preuves dans les pays étrangers ou auprès des familles.
⦁ Pérenniser l’action en participant financièrement à la formation de thérapeutes aux méthodes de rééducation neuro-motrice existantes en France, ainsi que la promotion des thérapies existantes dans d’autres pays
⦁ Par ailleurs l’association inscrit son projet dans une dimension d’intérêt général avec une ouverture au public international, notamment des plus fragiles, en préservant à ses activités un caractère non lucratif, laïque et apolitique. En toutes circonstances, l’association garantit un fonctionnement démocratique et transparent et préserve le caractère désintéressé de sa gestion.
Finally we have one orthopedic doctor in france who started to do SPML !
I post also hère in French :
Bonjour les parents juste je voulais vous dire que enfin il y a 1 médecin en france 🇫🇷 qui a commencé faire SPML ( opération orthopédique):
J’espère quelqu’en trouvera cet information utile :
On a rencontré médecin à Nice dr GHOUILEM en mai à Nice
qui justement a commencé opération SPML en france!
Cet opération nous – on a fait à Marc l’été dernier à usa ( C’est un seule enfant en france a ma connaissance qui était opéré par dr Nuzzo – et c’est lui qui a développé cet opération et pratiquer cet opération à usa 30 ans et il va bientôt partir à la retraite…) dr GHOUILEM est très ouvert esprits et était très content de rencontrer Marc .
Nous ont a fait SPML à Marc ete dernière à usa avec Dr Nuzzo : https://www.instagram.com/reel/Cq3y9z7NbZ6/?igshid=YmMyMTA2M2Y=
Qu’est ce que c’est SPML?
Un traitement chirurgical peu invasif pour les enfants atteints d’infirmité motrice cérébrale
Il s’agit d’une intervention chirurgicale réalisée sous anesthésie générale, au cours de laquelle le chirurgien allonge les muscles affectés par des trous pratiqués sur la peau et sur fascias!!! ( muscles pas coupé!)
Cette intervention ne nécessite pas de séjour à l’hôpital et le patient reprend rapidement sa thérapie et ses activités quotidiennes.
Méthode splm combinée à de l’éthanol Block
L’injection périneurale d’éthanol (« bloc d’alcool ») peut renforcer l’effet du SPML chez certains patients présentant un tonus accru et aussi pour enfants avec dystonia ( comme Marc).
Les 5 chirurgiens qui pratiquent cette Méthode combinée à de l ethanol block sont
– Dr Nuzzo inventeur de splm New Jersey
– Dr Yngve texas formé par nuzzo
– Dr Kanellipoulois formé par nuzzo (Grèce)
– Dr Bernius qui a également passé du temps avec nuzzo ( Allemagne)
Et Dr Price ( New York) – moi j’ai pas communiquer avec lui….
Dr David A. Yngve ( Texas) – contact :
mail: dyngve@utmb.edu
Dr Nuzzo New Jersey ( mais il doit partir à la retraite …. Que lui il retardé mais sa femme veut qu’il parte 😂 il a plus 70 ans mais c’est lui qui a développé SPML) ….
“Developed by RM Nuzzo, SPML differs from other orthopedic surgeries in its aims and procedures “
Contact Nuzzo :
video.popc@gmail.com
pediatric_orthopedics@yahoo.com
dr Kanellopoulos Grèce – contact:
info@adkanellopoulos.eu
Et Dr Bernius moi j’ai pas de mail j’ai communiquer via fb messanger
4 mai: on a rencontré un médecin chirurgien orthopédique à Nice Dr GHOUILEM qui s’intéresse de près à la Spml que le Dr Bernius a reçu cette semaine à Munich. Il veut amener la Spml en France. Il prévois aussi discuter avec Dr Kanellopoulos et en contact par mails avec Dr Yngve et Dr Nuzzo.
Nous avons échangé / bien discuté ( il m’a demandé si j’étais de métier 😂)….il a l’air très ouvert , que ça fait du bien de voir de tels médecins !! Avec qui on peut partager 🙂
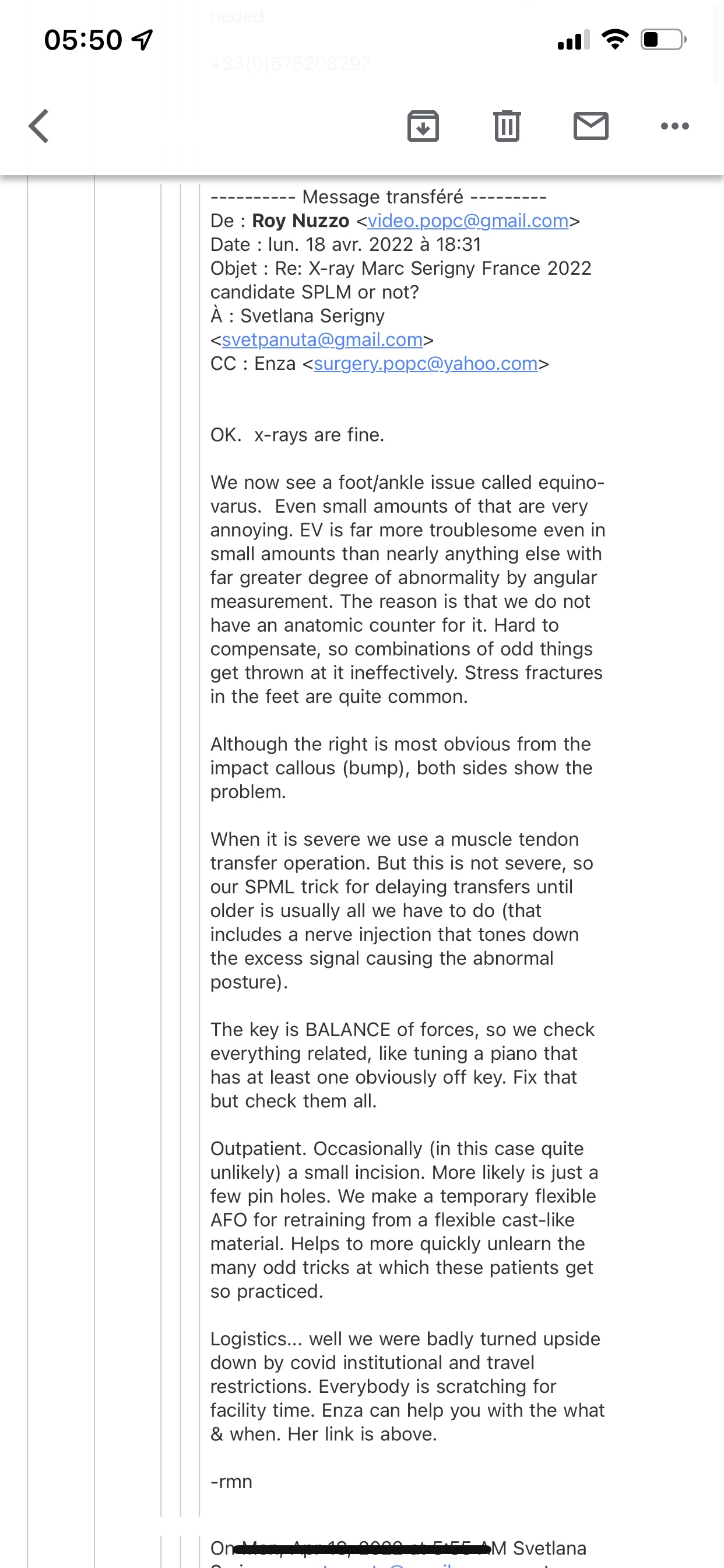
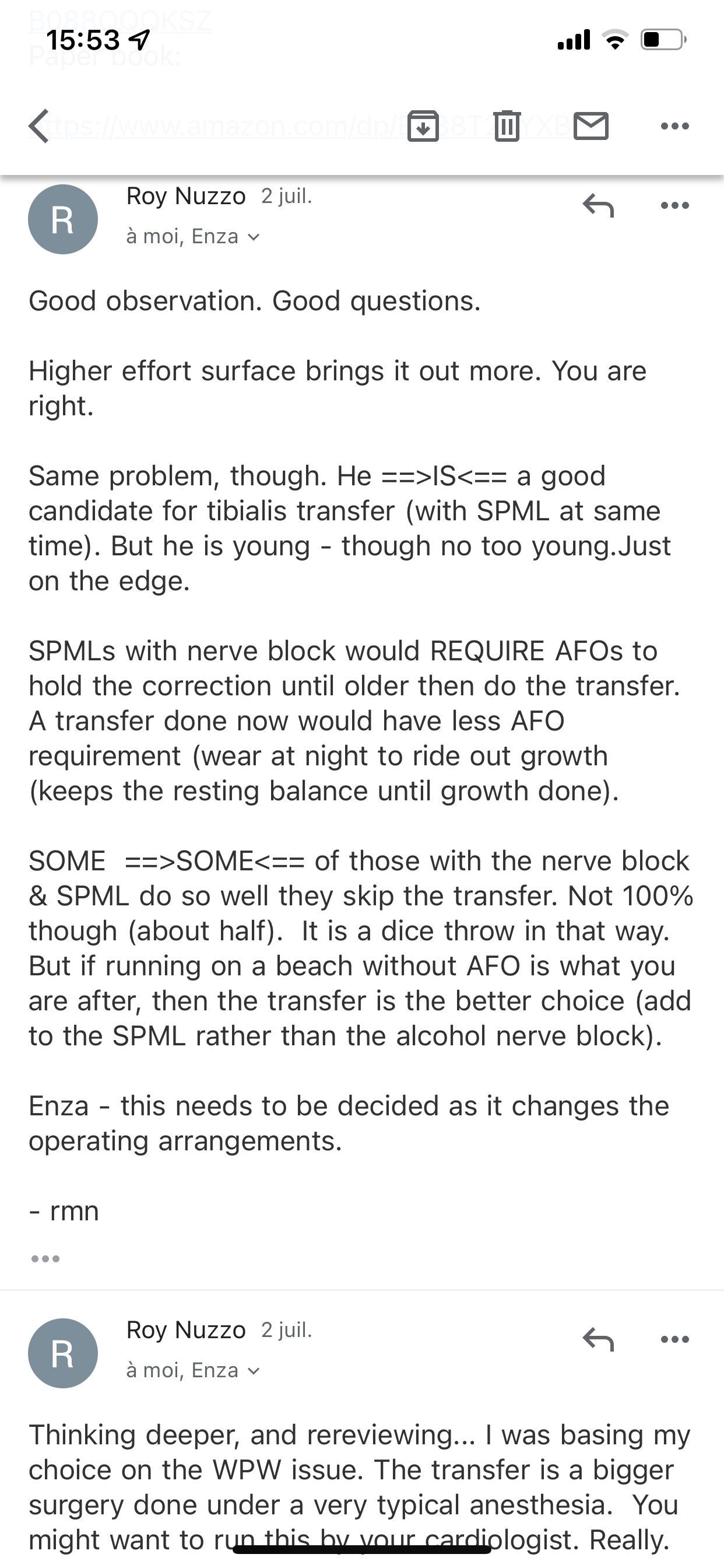
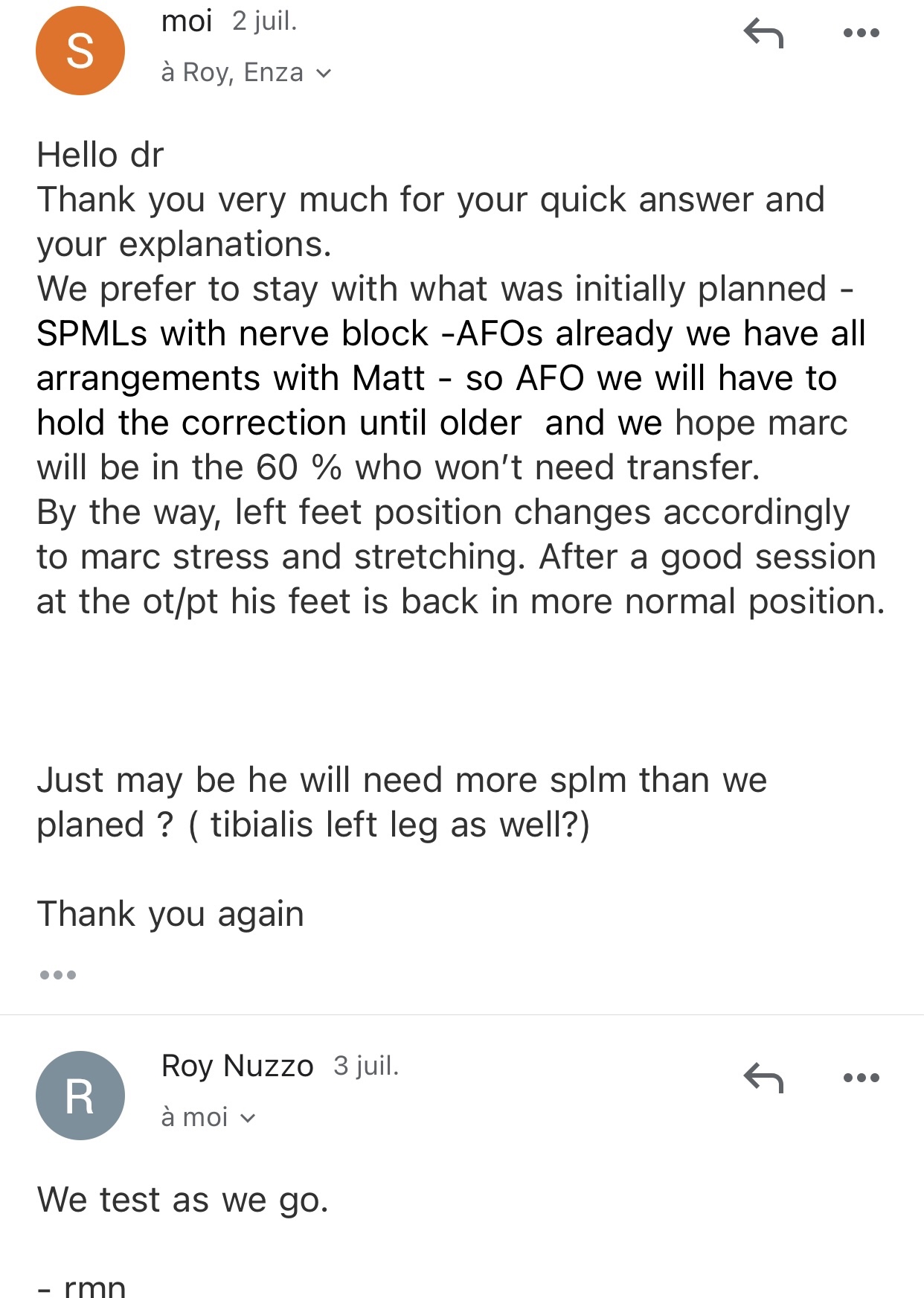
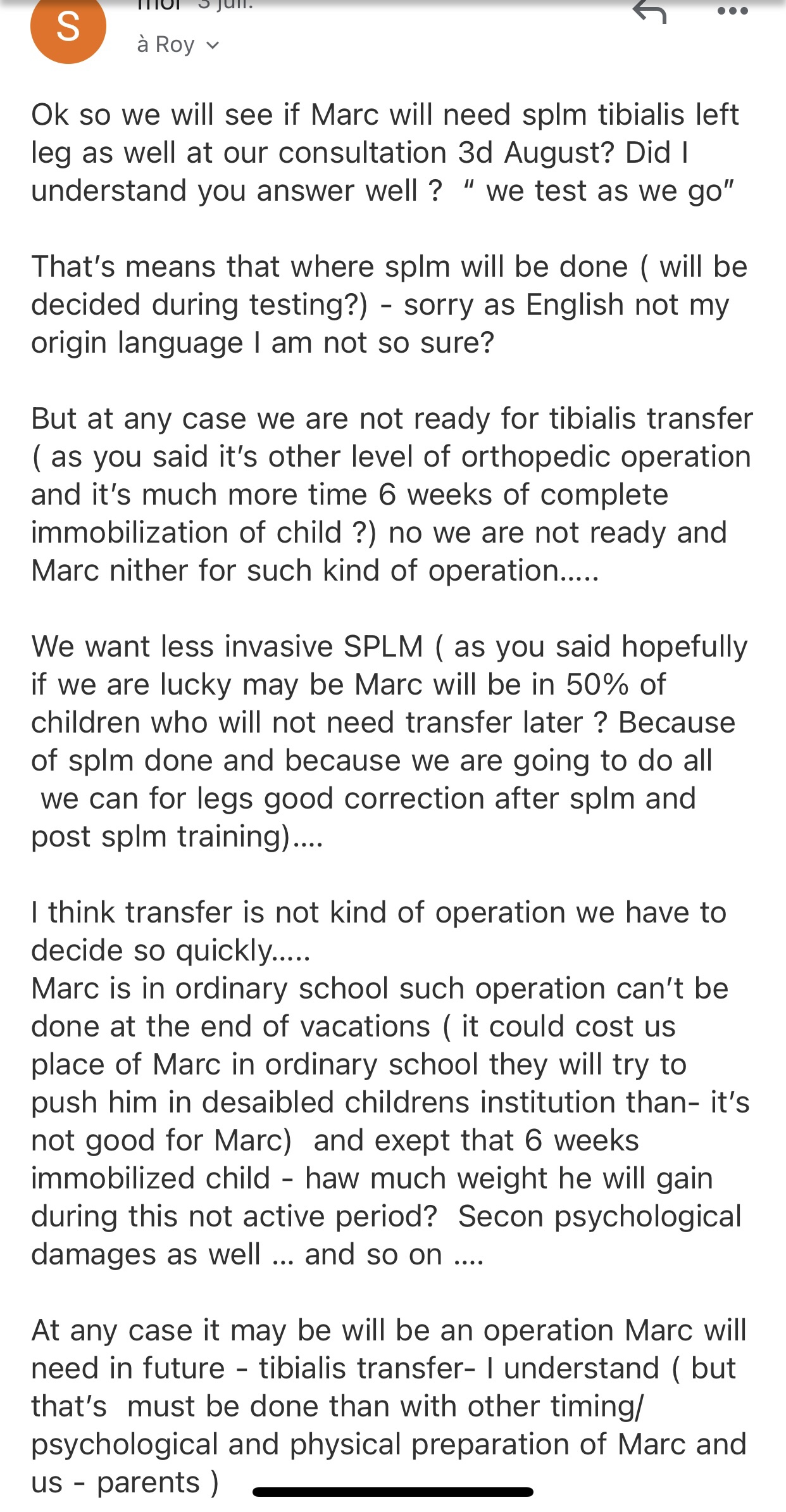
Acquired Spastic Equinovarus Deformity in case of my son Marc: ( in case of Marc we have also dystonia as well in his legs) .
Spastic equinovarus foot is due to spasticity and dystonia of the calf muscles (soleus, gastrocnemius and tibialis posterior), often complicated by contracture and by the weakness of peroneus longus and peroneus brevis muscles
2) second etude splm: https://www.researchgate.net/journal/Minimally-Invasive-Surgery-2090-1453/publication/343767239_Minimally_Invasive_SPML_Surgery_for_Children_with_Cerebral_Palsy_Program_Development/links/617bf69feef53e51e1009356/Minimally-Invasive-SPML-Surgery-for-Children-with-Cerebral-Palsy-Program-Development.pdf
3)Nuzzo :
R. M. Nuzzo, “SPMLs: selective percutaneous myofascial lengthening in velocity-dependant neuromuscular gamma-efferent high-gain feedback oscillation syndromes—or how I came to like the word “percs”,” Cerebral Palsy Magazine, vol. 2, no. 4, pp. 30–37, 2004.
Comparaison methode Ulzibat ( celle qui fait Nazarov en Espagne) et méthodes de Dr Nuzzo est mieux expliquer sur page de Dr Bernius : ( je crois en fb page tu peux choisir langue que tu veux ?)
So our operation it was ok till point of wake up … after that point It was difficult 😥
Marc was crying one leg didn’t support cast it was his dystonia…. We had to cut it off even before Nuzzo arrived back …..
It was very very difficult 😥
Dr Nuzzo he did new cast ( much looser) and open cast – dystonia of Marc not support real cust on his right leg
Left leg – he has no problems….
He had bad dystonia reaction on his right leg – soring/ temperature etc…. It was torture ….. ( I imagine not all patients has it) because boy before us from Canada was absolutely ok at getting out from hospital it was us – extreme crying and pain…
Doctor Nuzzo came back for us to hospital 40 minutes later …( we had to take off cast with nurses before he come back in urgency and it helped instantly) …. Yes as soon as we cut off his cast it helped instantly my son come from crazy crying to smiling ! Honestly !
Dr Nuzzo was escorted by police to get back quickly ….
He did new cast ( pre opened) which I can took off and he explained about dystonia…
It was difficult day I can’t tell it otherwise
Hopefully we will have results
For moment marc is just resting and don’t want to walk even to toilet
He did vomited also ( all around our hotel room) this i think Anestesia reaction…
( after vomiting feels better)….
1st day after operation :
He is better ( not yet walking ) but better he is in good mood
I can see his foots are really in stright position ( yes it’s impressive !) haw position of foot’s changed
So for naw we are just waiting when he has less pain in right foot ( to bear weight)
He can stand on his left foot but not right foot yet ( this one yet a bit hotter than left one and a bit more swollen)
So we take all with patience and give some time to Marc to recover.
2 d day after operation
Marc did 5/6 steps with help of his parents both side till toilet !
Yes it takes time to ré walking …
He also can walk 10-20 meters with Alinker bike help
Upset stomach this day ( may be medications during operation?)
3d day after operation:
We visited Atlantic City it was nice but a bit tired at end
I found his right leg more swollen after much walking….( on bike Alinker) but still it’s a lot of effects for transfers/ and some steps around bass in our hotel room – not real “ walking yet “
4 th day
Not yet “independently walking “
He could walking till toilet with my help one side this morning
And with helps of father :
5th day: starting walking with helps of our hends but we can go naw to our breakfast without Alinker
First steps indépendantly in room but still he is affraid to restart walking by himself :
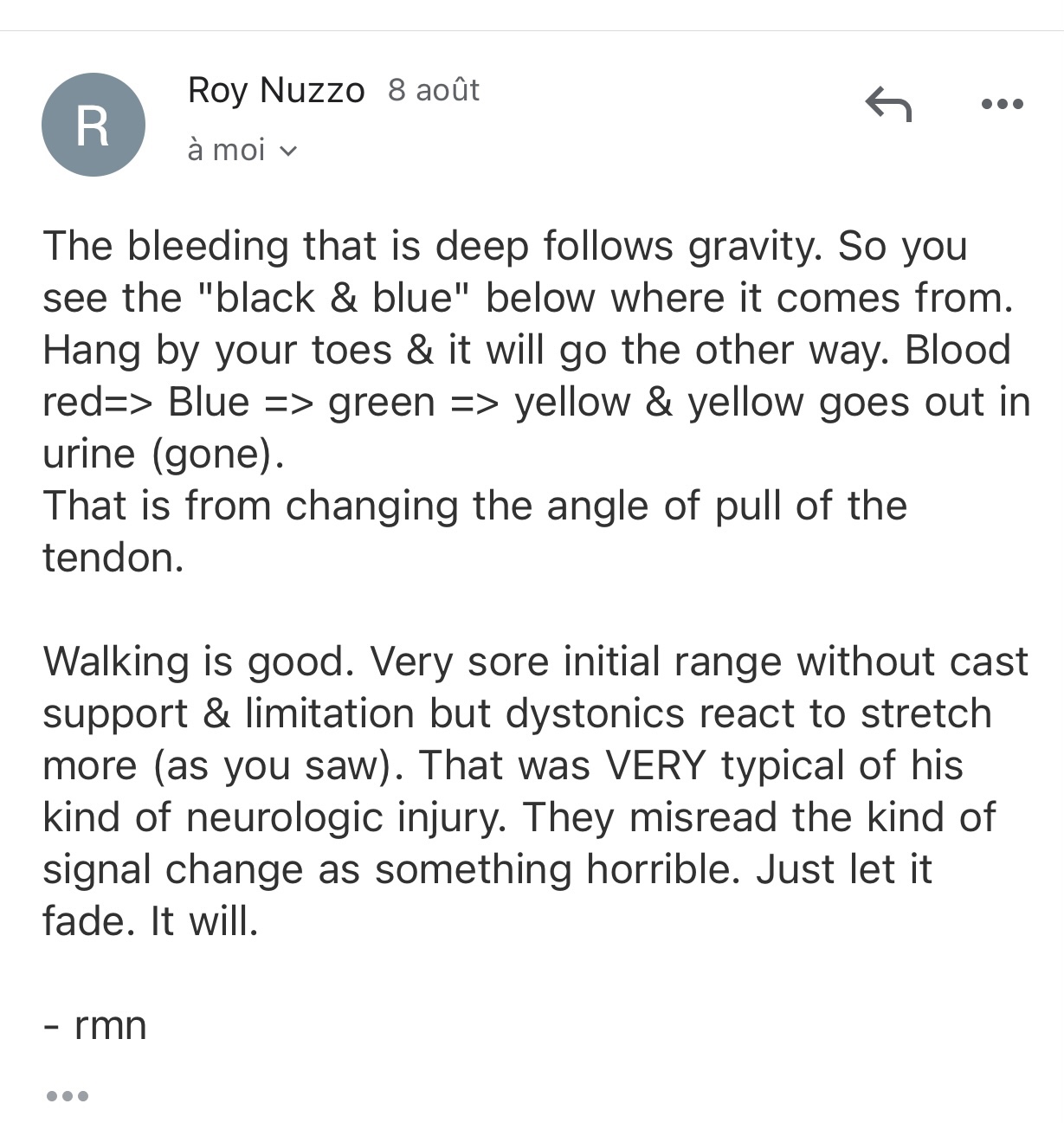
A lot of blue marks on foots and still pain in foots.
6 day :
Can walking a bit without holding but still bad balance and dystonia planing tricks so he stress and can lose control …
A lot of bike training but not much walking without Alinker…. (50 meters ? Before splm my son could walk independently 800 meters at least)….. so not yet at point of pre- operation level of independence – can’t go to toilet alone – can’t clean his teeth alone as before – not yet…
Dr Nuzzo said me that’s because in case of Marc it’s dystonia ( so not the same as spasticity and that’s why we saw big reaction to cast on his right leg had to cut asap just after operation and as soon as we took off cast on left leg – also dystonia reaction – left leg was teurning inside – it was heurting ) naw he is making used about all this changes – so not so much dystonic reactions as I put back his casts and bandages them……
Tomorrow we are getting his AFO
Hope it will help
I think if he had no pain and this blues he started to walking even better alredy …( but he has it may be need 2-3 weeks to pass all this swallowing and blues…)
7 day:
Marc has started slowly walking with the AFOs.
He says he feels like walking on his heels. As I see it, it is a bit like walking with ski shoes. As I understood, the angle is meant to be this way so he bends more his knees and uses his hips more. But this gives him a strange posture. And he is claiming it’s “not confortable” he is walking worse with AFO than he was walking with casts is it normal?….
It’s first day with AFO may be he need to be used to them but it’s strange that in AFOs he is less confidence than in casts he had….. he can’t walking even some steps independently again in afos….
While on casts he alredy did ….
Exept that these afos is so large it was really difficult to find shoes and he can’t do any more bike ( We’ve tried the training bike, something he likes to do and he is motivated by, but the AFOS are too large for the pedals.)
8 th day – coming back to France
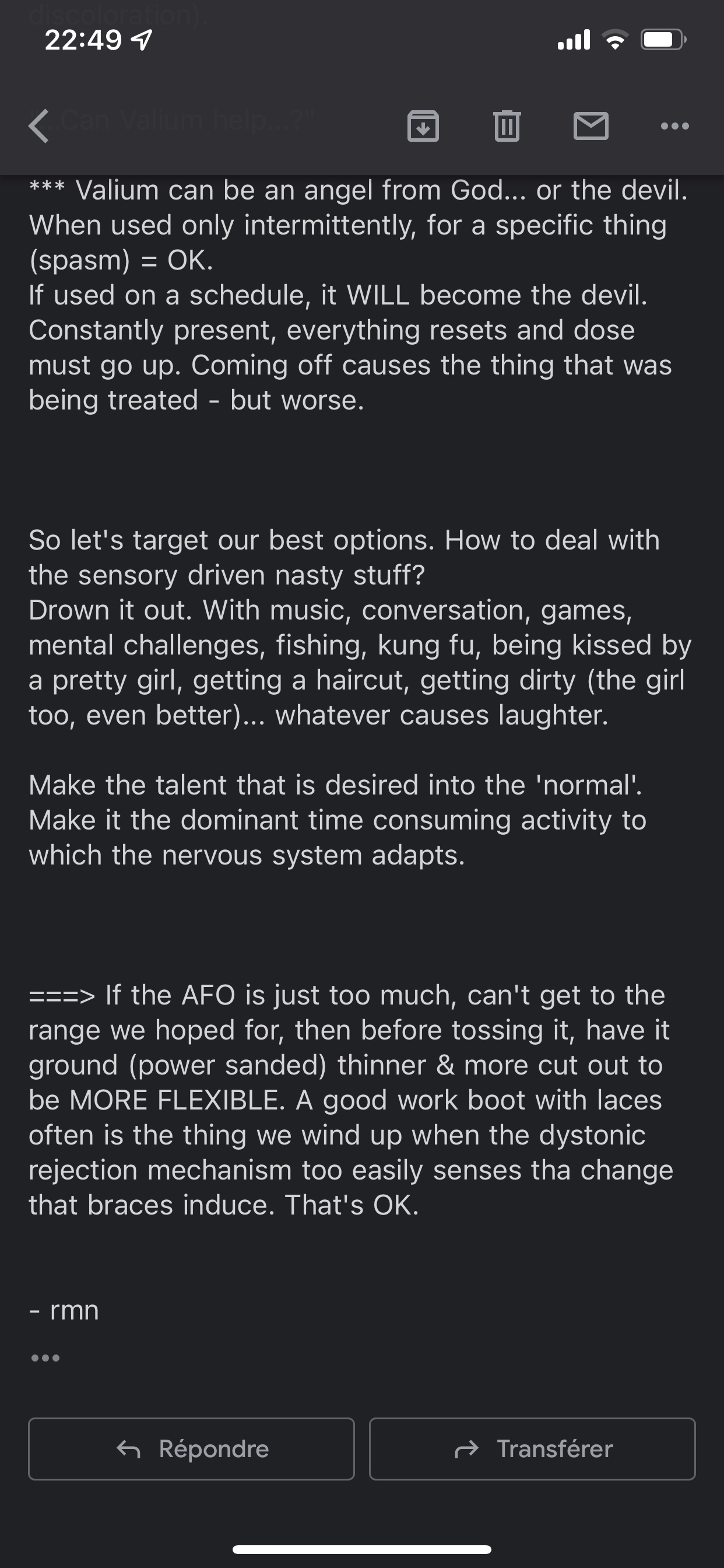
I was terrible traveling back to france I don’t know why but it was the worst day after surgery ( marc had spasms) I gave Valium it helped only a bit…
Marc still complains and mainly the arc of the foot and he had spams during all travel ( it was very difficult on the plain he was crying as well)
I gave Valium and paracetamol but it helped only a bit
I had to take off his AFOs ( for me it looks like it’s really related to the position of his foots in AFO) when I dance with the hills on my shooses 12 cm during all night I also has spasms and can’t were hill for sometime after … if you see what I mean ?
So I don’t know what to do?
Marc even asked me his casts back ( he was obviously better in casts than AFOs but I done have them of cause….we left them at. marc office when we took AFOs)….
Réaction after just 1 day wearing AFOs is really conserning for me … ( I understand that all of the work he has been doing of practicing walking and exercising new muscles in new ways, is equivalent to someone going to do heavy workouts at the gym everyday. his muscles can sore and may spasm. it is part of the healing process… but this is real regression again – not walking at all steaming and refuse to put afos
He is not even giving me to touch his legs! Even touching heurts….)
I live him naw to sleeping after very very difficult travel ( most difficult in my life I think…)
And I need advice:
What I have to do?
We don’t how much he is in pain exactly
He has walked day before travel quite a lot with his afos . Maybe 30/45 minutes altogether
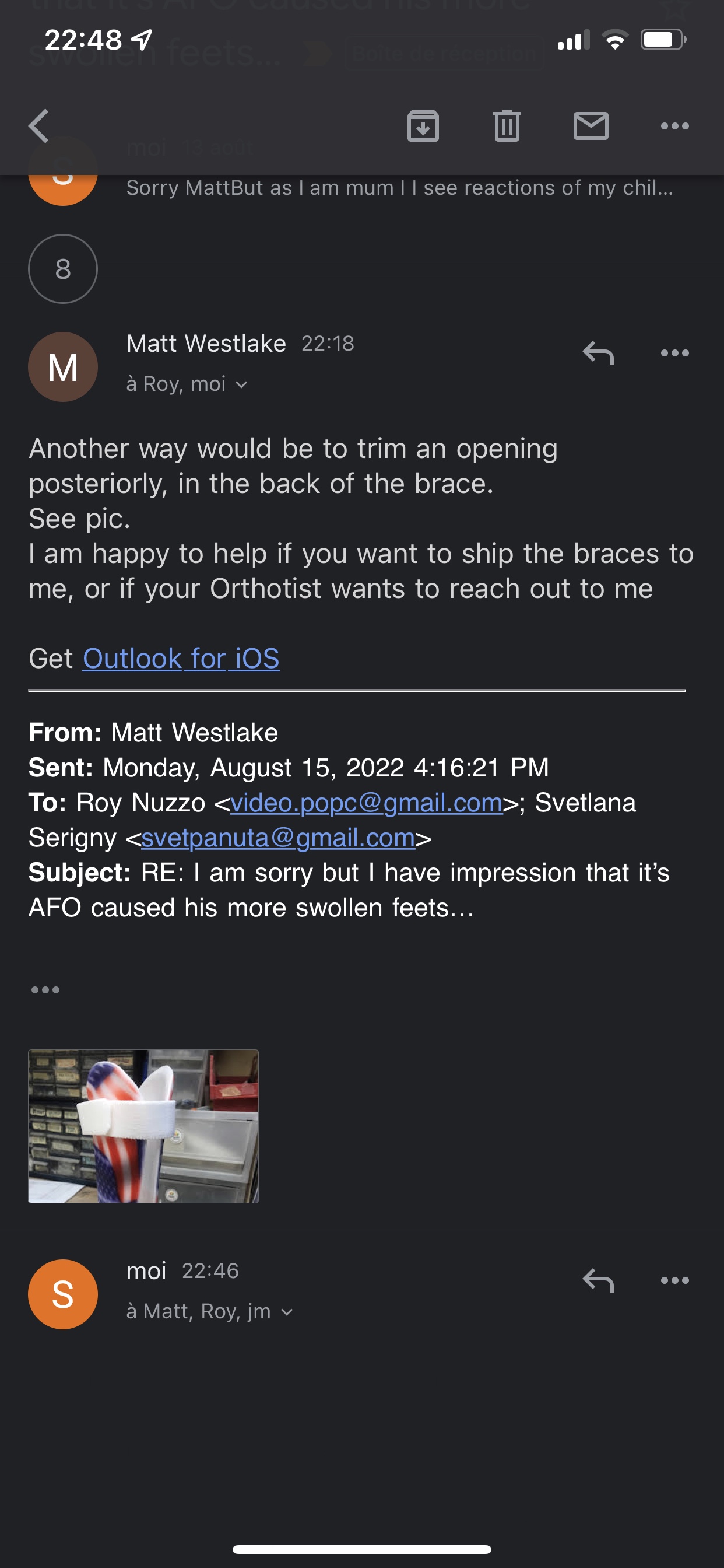
But even in the evening I found his feet more swollen and touching his ankles hurts him more than before AFOs….
May be instead of AFO I can use his old orthopedic shooses?
I don’t know…..
10 th day after operation
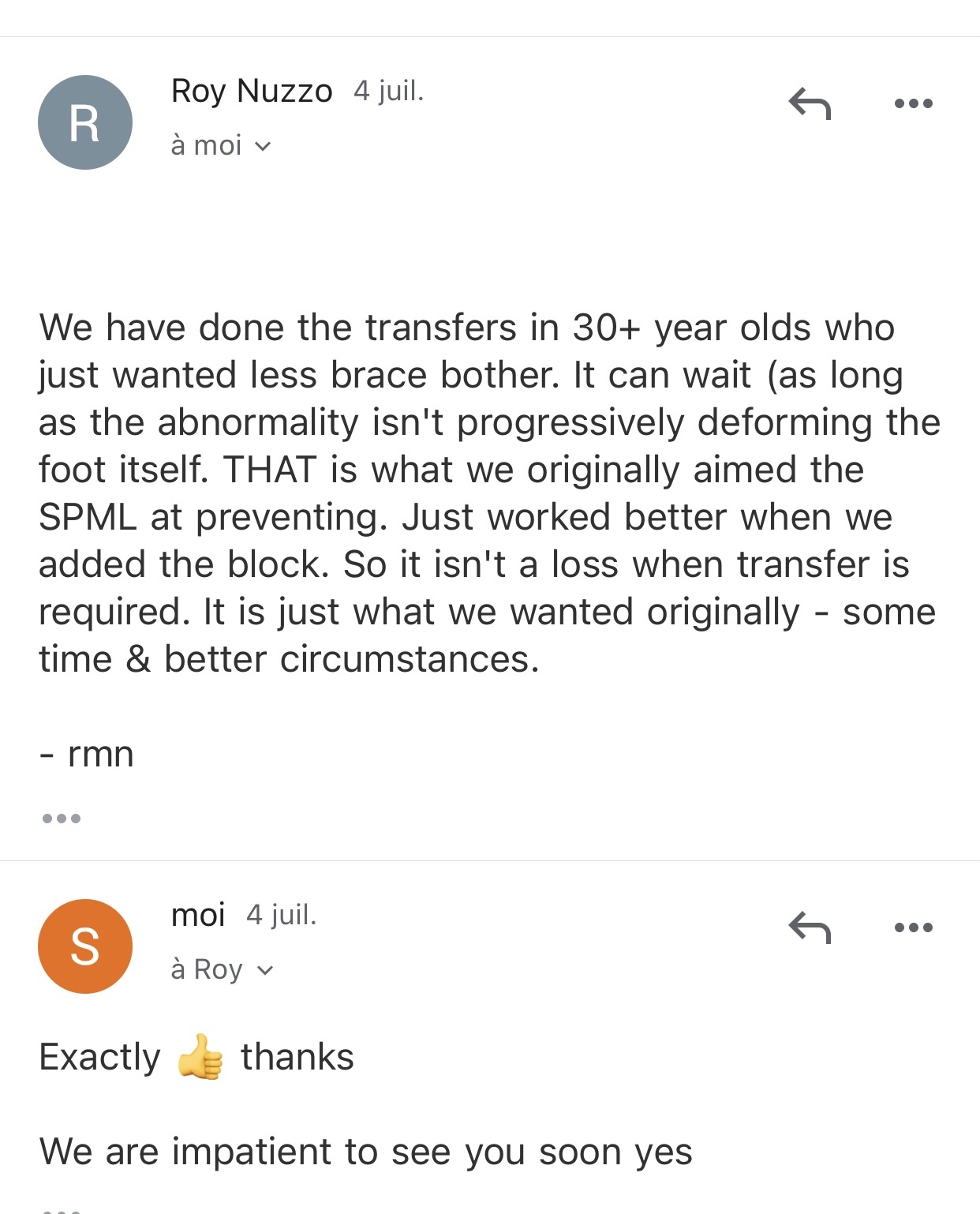
Finally I got answers from dr Nuzzo and Matt ( orthopedic dr):


12 th day after operation
What is important that he is better today 48 hours without right AFO and just small use of left AFO ( only in static positions) siting/ lying etc … Obviously his foots position improved enormously
So ….we will continue Feldenkrais will walking with ordinary boots and will see what orthopedic dr in france will say 22 August….about AFOs
18 days after splm:
20 days after splm:
https://youtu.be/dPv1qTf-HIM
So at any case his dystonia foot ( right still didn’t acsepted AFO after opening) so we stopped to use right AFO and just use left one while sitting ( watching tv or playing Xbox) and use Boots while walking : ( as dr Nuzzo advice)

some last videos of his progress : 22 and 23 days after Splm:
( at the stage you get person number you need to send NEW mail with number given) ! I did mistake to answer previous mail don’t repeat my mistakes 😉
So here instruction ver explicit : ( read well all points)
NSTRUCTIONS FOR TRANSFER OF INFORMATION BY EMAIL FOR CLINICAL TESTS
Email ct@cordbank.ru is designed for patients participating or planning to participate in clinical trials at the Dynasty Medical Center.
Sending messages to this e-mail indicates that you agree to the transmission of data, medical and other personal information via an open (unprotected by special means) communication channel.
Email is set up to help the researcher sort the letters and respond to them in a timely manner. When contacting the email address ct@cordbank.ru must follow the next rules, in case of the rules are not met, the researcher does not guarantee a response to the letter.
Incoming emails are processed in English and Russian, dates are displayed in DD / MM / YYYY format:
1. PRIMARY REQUEST FOR CLINICAL TESTS.
For the initial request for clinical trials, a letter should be sent to the researcher with the following heading:
PRIMARY _ CT _ REQUEST _ XX ,
Where XX indicate the clinical trial option: CP for cerebral palsy, AU – for autism;
Inside the letter you must provide the following information on the form:
Additionally, we request (this will help us to quickly determine the possibility of treatment) the most complete information about: is current medical condition of the patient, a brief description any held treatment and its effectiveness.
Further correspondence is conducted by replying to the previous letter so that the history of the correspondence is not interrupted. Please do not manually change the message header, do not send repeated requests and do not send new emails with attachments. If you are included in the study, you will be given a number with which you will continue to correspond with the researcher (see point 2).
2. FOR PATIENTS AT THE FIRST STAGE OF CLINICAL STUDY (SELECTION)
Patients included in the first stage of the study (selection) receive from the researcher an individual number that will need to be reflected in the title. Please make a NEW email with a NEW header. The new header will automatically sort your letters in the working group. Please write the first letter after entering the first stage of a clinical trial according to the following pattern:
CT_XX_S1 NNN,
Where XX – clinical trial option: CP for cerebral palsy, AU – for autism; NNN – a unique individual
number assigned to you by the researcher.
Patients can ask questions; send the requested documents (pdf, jpeg) at any time. Further correspondence is conducted by replying to the previous letter so that the history of the correspondence is not interrupted. Please do not manually change the message header, do not send repeated requests and do not send new emails with attachments.
Name of the patient
Date of Birth
Diagnosis
dates of diagnosis
Patient weight
Level GMFCS or ATEC
3. FOR PATIENTS ON THE SECOND AND THE THIRD STAGE OF A CLINICAL RESEARCH (SELECTION OF A GROUP AND PROCEDURE FOR THE INTRODUCTION OF CELLS).
After you have been assigned to the first or second study groups, and later, throughout the duration of the procedures, you can communicate with the researcher at any time on the topic of the clinical study. In order for you to receive prompt responses, you should change the subject of the heading in the following pattern:
CT _ XX _ S 2-3 NNN,
Where XX – clinical trial option: CP for cerebral palsy, AU – for autism; NNN – a unique individual
number assigned to you by the researcher in the second stage.
4. AFTER CONDUCTING THE INTRODUCTION OF CELLS.
After the first infusion of cells, the second infusion and until the end of the study, patients should transmit information about the effectiveness of treatment, for this, it is necessary to arrange the letter header as follows:
CT _ XX _ S 4 NNN,
Where XX – clinical trial option: CP for cerebral palsy, AU – for autism; NNN – a unique individual
number assigned to you by the researcher in the second stage.
All subsequent letters with research results should be sent in response to the first letter, without changing the title. Any questions or events about undesirable reactions should be sent to the researcher with such a title.
Инструкция по передачи информации по электронной почте для клинических испытаний. V003.02072019
( at the stage you get person number you need to send NEW mail with number given) ! I did mistake to answer previous mail don’t repeat my mistakes 😉
So here instruction ver explicit : ( read well all points)
NSTRUCTIONS FOR TRANSFER OF INFORMATION BY EMAIL FOR CLINICAL TESTS
Email ct@cordbank.ru is designed for patients participating or planning to participate in clinical trials at the Dynasty Medical Center.
Sending messages to this e-mail indicates that you agree to the transmission of data, medical and other personal information via an open (unprotected by special means) communication channel.
Email is set up to help the researcher sort the letters and respond to them in a timely manner. When contacting the email address ct@cordbank.ru must follow the next rules, in case of the rules are not met, the researcher does not guarantee a response to the letter.
Incoming emails are processed in English and Russian, dates are displayed in DD / MM / YYYY format:
1. PRIMARY REQUEST FOR CLINICAL TESTS.
For the initial request for clinical trials, a letter should be sent to the researcher with the following heading:
PRIMARY _ CT _ REQUEST _ XX ,
Where XX indicate the clinical trial option: CP for cerebral palsy, AU – for autism;
Inside the letter you must provide the following information on the form:
Additionally, we request (this will help us to quickly determine the possibility of treatment) the most complete information about: is current medical condition of the patient, a brief description any held treatment and its effectiveness.
Further correspondence is conducted by replying to the previous letter so that the history of the correspondence is not interrupted. Please do not manually change the message header, do not send repeated requests and do not send new emails with attachments. If you are included in the study, you will be given a number with which you will continue to correspond with the researcher (see point 2).
2. FOR PATIENTS AT THE FIRST STAGE OF CLINICAL STUDY (SELECTION)
Patients included in the first stage of the study (selection) receive from the researcher an individual number that will need to be reflected in the title. Please make a NEW email with a NEW header. The new header will automatically sort your letters in the working group. Please write the first letter after entering the first stage of a clinical trial according to the following pattern:
CT_XX_S1 NNN,
Where XX – clinical trial option: CP for cerebral palsy, AU – for autism; NNN – a unique individual
number assigned to you by the researcher.
Patients can ask questions; send the requested documents (pdf, jpeg) at any time. Further correspondence is conducted by replying to the previous letter so that the history of the correspondence is not interrupted. Please do not manually change the message header, do not send repeated requests and do not send new emails with attachments.
Name of the patient
Date of Birth
Diagnosis
dates of diagnosis
Patient weight
Level GMFCS or ATEC
3. FOR PATIENTS ON THE SECOND AND THE THIRD STAGE OF A CLINICAL RESEARCH (SELECTION OF A GROUP AND PROCEDURE FOR THE INTRODUCTION OF CELLS).
After you have been assigned to the first or second study groups, and later, throughout the duration of the procedures, you can communicate with the researcher at any time on the topic of the clinical study. In order for you to receive prompt responses, you should change the subject of the heading in the following pattern:
CT _ XX _ S 2-3 NNN,
Where XX – clinical trial option: CP for cerebral palsy, AU – for autism; NNN – a unique individual
number assigned to you by the researcher in the second stage.
4. AFTER CONDUCTING THE INTRODUCTION OF CELLS.
After the first infusion of cells, the second infusion and until the end of the study, patients should transmit information about the effectiveness of treatment, for this, it is necessary to arrange the letter header as follows:
CT _ XX _ S 4 NNN,
Where XX – clinical trial option: CP for cerebral palsy, AU – for autism; NNN – a unique individual
number assigned to you by the researcher in the second stage.
All subsequent letters with research results should be sent in response to the first letter, without changing the title. Any questions or events about undesirable reactions should be sent to the researcher with such a title.
Инструкция по передачи информации по электронной почте для клинических испытаний. V003.02072019
I am sorry I am brain injured child mum so i am scepical and veru critical… ok? So this is just my thoughts about Neuralink presentation:
1)Cortical only level for naw ( they don’t go yet deeper)?
2)Elon Musk Neuralink haw much he gains 2020?
3) I am sorry that I am so critical but I am firsthand want to see proofs that it’s works ? To put in head of healthy pigs don’t prove anything to me ?
Not into paralyzed pigs ?!
4) Honestly he was talking about deep brain stimulation ( at the beginning) I personally know 3 children’s – the inventor of DBS is french neurochirurgien -as I was told – (professeur Philippe COUBES ? )I met him – so in 3 children’s I know which had sdb by him – it’s in fact don’t work 2-3 years – after still searching level of stimulation neded ….
I don’t know even one person for whom it’s works DBS? there’s re a lot published studies and they are sayin it’s works…where they 150000 persons for who un it worked I am searching them for 2 years! ? Any testimonials?
they are giving technical briefings to bring in the best talent to bring this device to every person who needs it (great, but of course CEO Elon made $ 30,000 billion this year)?
Our brain is like an electrical network, and when it is damaged, it emits weak signals (but can electronics be compared to biology?) Neural communication amplifies weak signals (and much more in terms of reading and writing to the brain) and in the distant future will the tertiary level of the brain’s AI to do what the neural connection cannot do. Is this the largest technological and medical development since the 1800s. ????? I am not sure about this ….
Have they already got FDA approval for a breakthrough device? Is it money or real progress? An artificially implanted chip? I have a lot of questions and I am very careful about this …
All this is PR and money making? Better to promise to send people to Mars. It is normal to collect money from dreamers, but not from the sick.
Yes. Work is underway on impulse-controlled prostheses. And if you manage to decorate the signals, then you can mentally control some auxiliary devices. It is a well-known misconception that we can surpass our creator. It is enough to look at the medieval paintings of how they tried to make a man with the help of springs and gears.
They do not yet know how to translate the chemistry of the brain and thinking into a conscious binary code. While they can train a person to strain something and relax something simple. For example, take a glass of prostheses controlled by a brain impulse.
So it’s gives realistic perspective….
Also : « « Former employees told Stat News that the company was chaotic, and that researchers were under intense pressure to rush through projects. Scientists were sometimes given weeks to complete projects that should take months, for example. “They are building a medical device and a surgical approach to implant that medical device, and they’re approaching it with the use of a tech company — move fast and break things,” one employee said. »
« The announcement of the technology was based on two white papers published in bioRxiv, reports written by NeuraLink scientists and not peer-reviewed. In both published white papers, no attempt has been made to use the recorded neuronal data for the purposes of a BCI, and no attempts to simulate neurons through NeuraLink have been reported.
It’s fairly likely the company has achieved more than is reported in the white papers, the nature of scientific research being that breakthroughs are sometimes made years before they can be published. »
« Neuralink’s microscopically slender electrodes are designed to provide longer-term recording than current electrodes and produce less tissue damage, but it’s still not clear how this will stand up over time. In the first study cited, recordings were made from one rat implanted with the electrodes for 60 days, with the implants falling off prematurely in the other three rats studied.
By comparison, the Utah array has reported longevity of six to nine years when implanted into a primate brain. »
You see I eventually don’t use any my own words ….
Dr. Olga Tyumina is the President of Ruscord, a non-profit organization of specialists and organizations in the field of procurement, storage and use of umbilical cord blood and cellular technologies. Dr. Tyumina is a prominent doctor in medical sciences, professor of the Russian Academy of Sciences, honored health worker in the Samara Region (Russia), and the Director of the Samara Regional Medical Center, Dynasty. She is the author of 120 publications and holds multiple patents, registered computer programs and monographs.
Dr. Stanislav Volchkov is the Deputy Director of the Samara Regional Medical Center, Dynasty, the Executive Director of the non-profit Hematopoietic Progenitor Cells Registry, Expert of the Fund for Assistance to Small Innovative Enterprises in Science and Technology, Founder of the Institute of Biotechnology and Pharmacology Inbiopharma, LLC, and is a certified designee for biomedical cellular products acquired by Ministry of Health of the Russian Federation.
In this live chat we will discuss the clinical trials, future research, and treatments currently provided at the Center of Cellular Technologies in Samara (Russia) using donor cord-blood transfusions and other stem cell therapies for the treatment of Autism, Cerebral Palsy and other developmental disorders.
In 2020 it was big pose ( because of Covid) and we decided as we can’t travel we bought Galileo plate…
In july 2020 I think somthing like that ( I don’t remember exactly date ) we didn’t use it a lot before our travel to center BrainMoove (end July 1 week ) but after our reteurn – Every day Galileo end August and September….
And Marc did stoped walking in October! And he was complaining about pain at same time yes he fall at school ( but finally naw with time I know it was Galileo plate – not the fall responsible)….
also just to add about Galileo plate ( my son good walker was using about 1 month a bit more …may be but in beginning of October … he stoped Walking and complained about pain ! We did radios and a lot of consultations and foud that his legs become much more stiffer than before ( why ? What the reason of spasticity just augmented so quickly and enormously?)
I was searching a lot it happened last year ) so I foud yes it could damage as well ( in standing position) he had pain in tibias posterior! – And guess what Dr Nuzzo will be operating him during splm? – on tibias posterior…. It’s augmented his stiffness enormously honestly – it took me 2 weeks intensive PT that he just restart to walking ( not as well as before) and about 3 months training that he approximately achieve his previous Level ( before starting Galileo) so it was our very bad experience – Galileo honestly…. He still didn’t achieve same level on stairs as before Galileo – so it’s one of mistakes I did and it was ours bad experience )….
“More significant adverse effects have also been reported including hip (Crewther et al., 2004) and knee pain Russo et al., 2003), and discomfort from the vibration induced head motion (Crewther et al., 2004). One study (Cronin, Oliver & McNair, 2004) reported participants to complain of pain in the jaw, neck, and the lower extremity (particularly in the tibialis posterior). The pain required physiotherapy treatment in some participants and took seven to ten days to subside.”
While it is known that Ia afferents inhibit motor neurons to the antagonistic muscle (Mester et al. 1999), vibration also induces a tonic vibration reflex (TVR) and increases muscle stiffness (Cronin et al. 2004;Mester et al. 1999).
« Researchers at Lyndhurst Centre caution that Whole Body Vibration may elicit inner ear troubles, dizziness, headache, lower-limb spasticity, fracture (especially among those with severe osteoporosis), and/or hardware loosening (plates or screws as a result of surgery).(20) »
July 2020 – 1 weeksGyrostim and neroplasticity brain center training 3h per day
so studies when it can cause problems:
1)“More significant adverse effects have also been reported including hip (Crewther et al., 2004) and knee pain Russo et al., 2003), and discomfort from the vibration induced head motion (Crewther et al., 2004). One study (Cronin, Oliver & McNair, 2004) reported participants to complain of pain in the jaw, neck, and the lower extremity (particularly in the tibialis posterior). The pain required physiotherapy treatment in some participants and took seven to ten days to subside.”
While it is known that Ia afferents inhibit motor neurons to the antagonistic muscle (Mester et al. 1999), vibration also induces a tonic vibration reflex (TVR) and increases muscle stiffness (Cronin et al. 2004;Mester et al. 1999).
2)« Researchers at Lyndhurst Centre caution that Whole Body Vibration may elicit inner ear troubles, dizziness, headache, lower-limb spasticity, fracture (especially among those with severe osteoporosis), and/or hardware loosening (plates or screws as a result of surgery).(20) »
3)Cardiovascular Stress Induced by Whole-Body Vibration Exercise in Individuals With Chronic Stroke : https://academic.oup.com/ptj/article/95/7/966/2686433
Normalement ils avez même pas le droit de nous vendre Galileo a cause que Marc a au aret cardiaque ….a 4 ans
4) this study showed that application of WBV to chronic stroke patients was not helpful for improving their immediate balance ability. The adverse effects of WBV have been reported in previous studies:
Whole body vibration may have immediate adverse effects on the postural sway of stroke patients
but hère good studies about :
Dernière étude 2019: The immediate influence of various whole-body vibration frequency on balance and walking ability in children with cerebral palsy: a pilot study:
« Le WBVT fourni par Galileo plate est caractérisé par des mouvements de bascule qui stimulent un modèle de mouvement similaire à la démarche humaine. Celles-ci entraînent l’activation de circuits vertébraux propriétaires-réceptifs, conduisant ainsi à des contractions musculaires rythmiques compensatoires dans les membres inférieurs et le tronc. Nos participants ont non seulement affiché des améliorations de la masse musculaire, mais également des améliorations de la teneur en minéraux osseux et de la densité allant de 1 à 5%. L’augmentation de la masse osseuse était probablement due à l’effet de l’action musculaire sur l’os pendant le WBVT, combiné aux effets de l’amélioration de la mobilité observée. Ainsi, nos résultats cadrent bien avec la théorie du mécanostat, dans laquelle la charge mécanique (dans ce cas, les contractions musculaires générées par la plate-forme de vibration et l’amélioration de la mobilité) a entraîné des effets positifs sur les os, tels qu’une augmentation de la masse osseuse. Notez que nos résultats étaient similaires à ceux observés par Stark et al. après 6 mois de thérapie combinée dans un groupe de 78 enfants atteints de GMFCS I à V, qui ont rapporté respectivement une augmentation de 2,3% et 5,7% de la densité et de la teneur totale en minéraux osseux. Cependant, leur intervention impliquait non seulement le WBVT, mais aussi d’autres formes de physiothérapie, de musculation et d’entraînement sur tapis roulant, ce qui rendait impossible l’identification des effets spécifiques du WBVT. Néanmoins, Wren et al. ont examiné l’impact de l’entraînement quotidien aux vibrations seul sur la santé osseuse des enfants atteints de PC âgés de 6 à 12 ans, observant des améliorations de la zone osseuse corticale par rapport à un régime de simplement se tenir debout sur le sol8.
https://www.nature.com/articles/srep22518.pdf
https://www.nature.com/articles/srep22518
Alinker: ( vélo – debout) pour marcher ( Marc manque encore 2 cm longueur des jambes)