
HBOT (Hyperbaric Oxygen Therapy) is a medical treatment which is also used in autism/Cp /anoxic injury etc….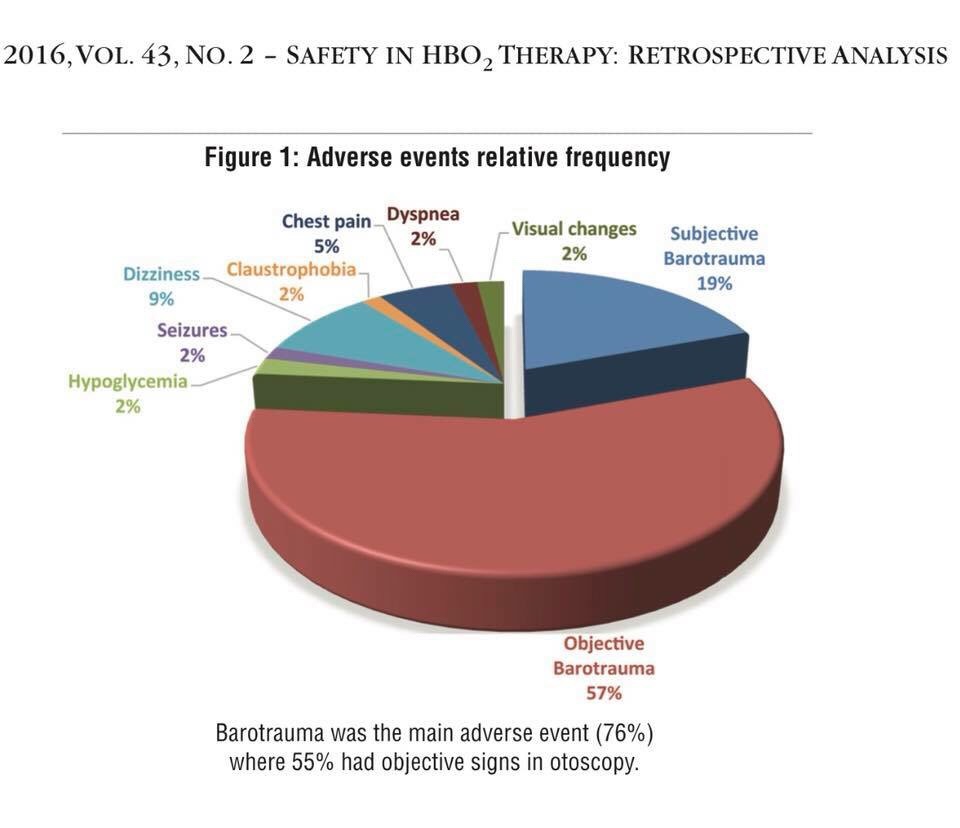
The safety of hyperbaric oxygen treatment – retrospective analysis in 2,334 patients:
https://www.researchgate.net/profile/Shai_Efrati2/publication/303569636_The_safety_of_hyperbaric_oxygen_treatment_-_retrospective_analysis_in_2334_patients/links/5760cfdf08ae244d0370d4da/The-safety-of-hyperbaric-oxygen-treatment-retrospective-analysis-in-2-334-patients.pdf?origin=publication_detail
Oxygen could be toxic if not administered properly, so that’s why I want tell parents about this fact and I advice to take consultation with specialist ( of your choice) before any HBOT treatment ( whichever type of pressure or type of chambers you choose to use it’s safer if treatment monitored by HBOT doctor especially if supplemental oxygen is added)
Part I
Oxygen toxicity:
Protocols for the avoidance of hyperoxia exist in fields where oxygen is breathed at higher-than-normal partial pressures but protocol must be monitored.
But not much centers are doing complete check up ( as i am doing for Marc before/after HBOT)
EKG
Blood tests
Medical tests and checking his tubes and ears
Vision tests
His heart beats / pulse rate and pressure and oxymeter are measured, every day before/and after HBOT
So I know that he doesn’t get oxygen toxicity from his HBOT treatment.
Patients at risk for pulmonary oxygen toxicity should be monitored for oxygen saturation and increased work of breathing. They can be evaluated by pulmonary function testing and chest x-rays which can show signs of ARDS.
(In Israel we did X-Rays for marc and me(as we are going with him inside the chamber)
Similarly, eye exams assessing acuity and looking for lens opacification can be done to detect early ocular oxygen toxicity. (Also did all ayes tests before starting HBOT)
CNS toxicity manifests as described and will often have tachycardia and diaphoresis as well. (as well because my son condition is WPW = tachycardia possible in his case so this point and blood pressure is monitored every day)
Aborting a hyperbaric exposure when these signs are present can prevent seizure occurrence!!
So here or file with docs to read:
Oxygen Toxicity :
The effects of oxygen toxicity may be classified by the organs affected, producing three principal forms:
• Central nervous system, characterised by convulsions followed by unconsciousness, occurring under hyperbaric conditions;
• Pulmonary (lungs), characterised by difficulty in breathing and pain within the chest, occurring when breathing increased pressures of oxygen for extended periods;
• Ocular (retinopathic conditions), characterised by alterations to the eyes, occurring when breathing increased pressures of oxygen for extended periods.
Central nervous system oxygen toxicity can cause seizures, brief periods of rigidity followed by convulsions and unconsciousness, and is of concern to divers who encounter greater than atmospheric pressures. Pulmonary oxygen toxicity results in damage to the lungs, causing pain and difficulty in breathing. Oxidative damage to the eye may lead to myopia or partial detachment of the retina. Pulmonary and ocular damage are most likely to occur when supplemental oxygen is administered as part of a treatment, particularly to newborn infants, but are also a concern during hyperbaric oxygen therapy.
Oxygen toxicity seizures (Bert effect) can occur with hyperbaric oxygen therapy in a dose-dependent relationship. The overall risk may be as frequent as 1 in 2000 to 3000 treatments. However, this risk may be as high as 1 in 200 at higher pressures (2.8 to 3.0 times normal atmospheric pressure or one atmosphere absolute (ATA)) and as low as 1 in 10,000 for treatment at 2 ATA or less. One study looking at the hyperbaric treatment of decompression illnesses noted an overall incidence of oxygen toxicity events of 7%. The incidence of pulmonary toxicity (Smith effect) was 5%, while 2% for central nervous system symptoms, and a seizure rate of 0.6%.
Central nervous system signs and symptoms:
• Headache
• Irritability and anxiety
• Dizziness
• Disorientation
• Hyperventilation
• Hiccups
• Cold shivering
• Fatigue and restless ( difficulty to sleep)
• Tingling in the limbs
• Visual changes such as blurring and tunnel vision
• Tinnitus and Hearing disturbances
• Nausea
• Twitching
• Tonic–clonic seizure
Pulmonary toxicity signs and symptoms:
• Mild tickle sensation on inhalation
• Mild burning on inhalation
• Uncontrollable coughing
• Hemoptysis
• Dyspnea
• Rales
• Fever
• Hyperemia of the nasal mucosa
• CXR shows inflammation and pulmonary edema
Eyes:
• In premature babies, retinopathy of prematurity and retrolental fibroplasia
• Cataract formation (long-term exposure)
And now some studies about and links:
1) Several side effects and complications from hyperbaric oxygen (HBO2) therapy have been described, with varying degrees of seriousness. By far, the two most frequent and benign side effects comprise middle ear barotrauma, which has been noted in up to 2% of treated patients, and can be prevented or minimized by teaching autoinflation techniques, or by inserting tympanostomy tubes. Another frequent complaint is claustrophobia, both during multiplace and monoplace chamber compression, requiring reassurance, coaching and, at times, sedation. Other more rare, but more severe side effects derive from oxygen (O2) toxicity, from the multiple exposures required for chronic treatments, especially progressive myopia, usually transient and reversible after stopping HBO2 sessions, or pulmonary dyspnea, with cough and inspiratory pain. More serious O2-induced seizures happen rarely, at higher O2 pressures, and often during acute treatments in acidotic patients (carbon monoxide poisoning). Source :
https://www.ncbi.nlm.nih.gov/m/pubmed/24984321/
2)Oxygen delivered in supraphysiological amounts is currently under investigation as a therapy for brain injury. Hyperoxia can be delivered to the brain under normobaric as well as hyperbaric conditions. In this study the authors directly compare hyperbaric oxygen (HBO2) and normobaric hyperoxia (NBH) treatment effects.
And here if somebody wants to read comparaison bethween normobaric and hyperbaric oxygen toxicity :
( oh it’s TBI but the same processes we have for all human metabolism for others injuries as well….)
« Hyperbaric O2 has a more robust posttreatment effect than NBH on oxidative cerebral metabolism related to its ability to produce a brain tissue PO2 ≥ 200 mm Hg. However, it appears that O2 treatment for severe TBI is not an all or nothing phenomenon but represents a graduated effect. No signs of pulmonary or cerebral O2 toxicity were present. »
http://thejns.org/doi/abs/10.3171/2009.7.JNS09363
3)clinical trail of dr Harch for oxygen toxicity :
https://clinicaltrials.gov/ct2/show/NCT00592891
4)
And here about oxygen /hemoglobin etc
Under normobaric conditions, the majority of oxygen is transported within the erythrocytes bound to hemoglobin. Breathing of 100% oxygen already results in a 100% saturation of hemoglobin.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4666443/
5)Dr. J. Lorrain Smith first described the toxic effect of oxygen on the lungs in 1899. He noted that the severity of the effect increased with increasing pO2 and that the effects where largely reversible. As shown in the diagram, the toxic effects of oxygen at partial pressures between 0.45 ATA and 1.6 ATA are primarily on the lungs while the toxic effect at pO2s over 1.6 ATA are primarily on the brain.
The earliest sign of pulmonary (lung) oxygen toxicity is a mild irritation in the trachea (throat) that is made worse with deep inspiration. A mild cough develops next, followed by more severe irritation and cough until inspiration becomes quite painful and the cough becomes uncontrollable. If exposure to oxygen is continued, the person will notice chest tightness, difficulty breathing, shortness of breath, and if exposure is continued long enough, the person will die, from lack of oxygen! The progressive damage to the lungs eventually makes it impossible for the oxygen to get to the blood as it passes through the lungs. The time to onset of symptoms is highly variable but most individuals can tolerate 12-16 hours of oxygen at 1.0 ATA, 8-14 hours at 1.5 ATA, and 3-6 hours at 2.0 ATA before developing mild symptoms. There are several ways to track developing pulmonary oxygen toxicity but the most sensitive and accurate is the development of symptoms. A second technique is to monitor the vital capacity. Vital capacity (the amount of air that can be moved in one large breath) decreases with increasing pulmonary toxicity. A reduction of approximately 2% in vital capacity correlates with mild symptoms while a reduction of 10% correlates symptoms so severe that most individuals will not voluntarily continue breathing oxygen. These mild effects are completely reversible and no permanent lung damage occurs. However, the damage will take 2 to 4 weeks to heal. The pathology of pulmonary oxygen toxicity is understood but beyond the scope of this discussion.
A third way to keep track, in rough terms, of pulmonary oxygen toxicity is to keep track of the oxygen exposure. This technique is called calculating the Unit Pulmonary Toxic Dose (UPTD) and one UPTD is equivalent to breathing 100% oxygen, for one minute, at 1.0 ATA. As a guide, 615 UPTDs in one day will cause a 2% reduction in vital capacity and 1,425 units will cause a 10% decrease. There are several different ways to calculate the UPTD (some try to correct for increasing toxic effects with increasing dose, in addition to the simple pO2) and there is quite wide variation in individual tolerance so that symptoms are still the best guide. The situation where UPTDs are most useful is in planning a large number of dives, in a few days, all involving a large amount of oxygen decompression or CCR diving. Even then, the dive plan may have to be altered if the diver develops symptoms of pulmonary toxicity.
The first and most important method to prevent pulmonary oxygen toxicity is to limit exposure to the lowest possible pO2 for the shortest period of time.
The second method to prevent pulmonary oxygen toxicity is to provide air breaks.
https://www.diverite.com/articles/oxygen-toxicity-signs-and-symptoms/
Part II
HBOT fire security and obligations:
NFPA 99 2015 Chapter 14 Hyperbaric Facility
2012 NFPA Ch 14 student handout
Thanks Svetlana