PoNS
What is Pons?
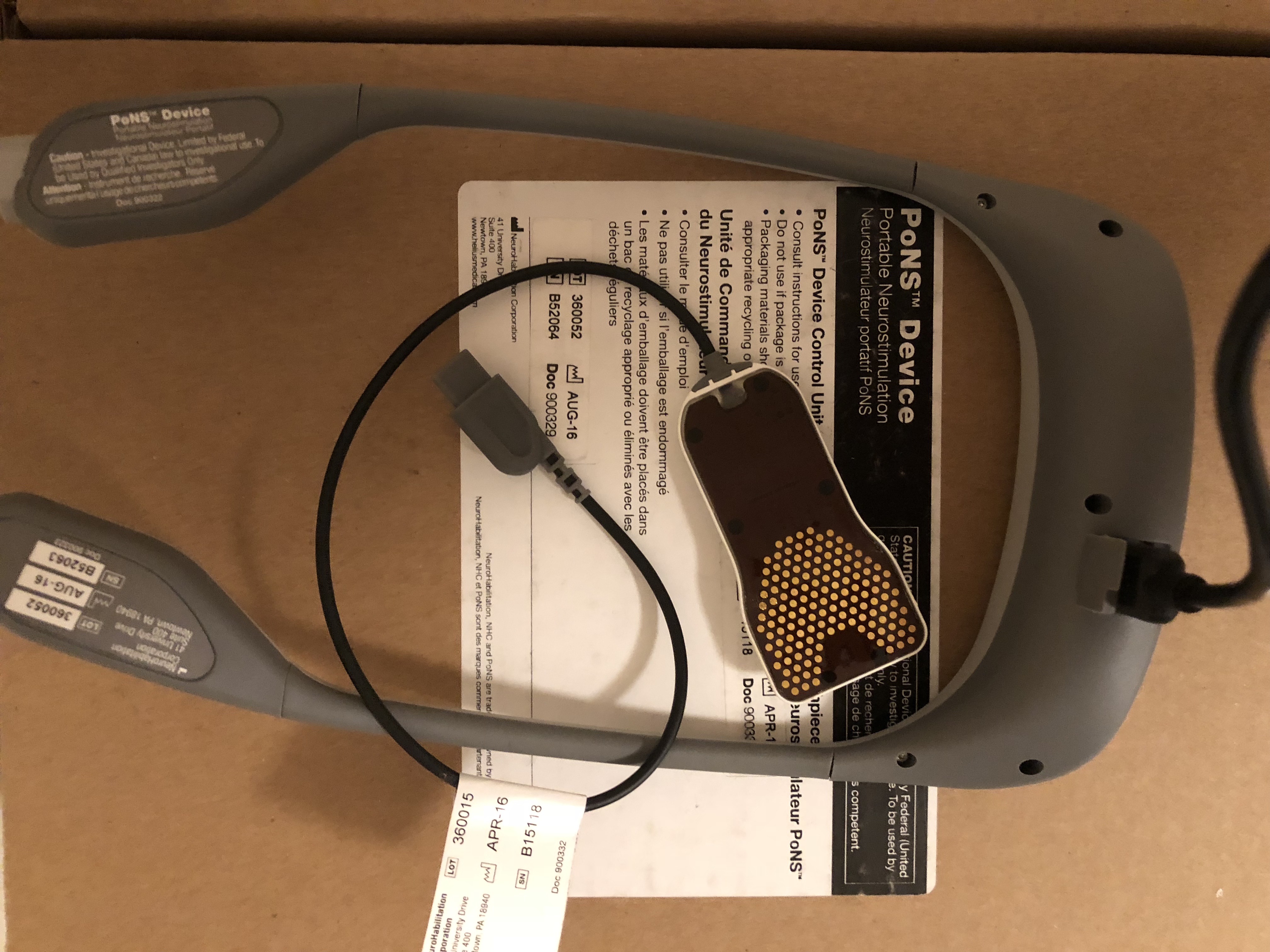
It’s a Device to help Cranial Nerve Non-Invasive NeuroModulation (CN-NINM) via the tongue:
The CN-NINM intervention is an experimental regimen. It has been developed over the last 12 years at Tactile Communication and Neurorehabilitation Laboratory (TCNL) at the University of Wisconsin – Madison. The PoNS™ is an experimental device that has been evolved over this same period at TCNL, PoNS receive 22 October 2018 Medical Device License Clearance from Health Canada but PoNS is not yet FDA approved.
NEWTOWN, Pa., Dec. 12, 2018 (GLOBE NEWSWIRE) — Helius Medical Technologies, Inc. (NASDAQ:HSDT) (TSX:HSM) (“Helius” or the “Company”), a neurotech company focused on neurological wellness, today announced that its wholly owned subsidiary, NeuroHabilitation Corporation, has submitted an application for a CE Mark, the receipt of which will allow the Company to market its Portable Neuromodulation Stimulator (PoNS™) in the European Union.
PoNS is a licensed class II medical device in Canada and an investigational medical device in the U.S. and the European Union.
https://heliusmedical.com/index.php/newsroom/news-release/2018/246-?utm_source=dlvr.it&utm_medium=facebook
About:
Waiting FDA clearance :
So:
The PoNS (portable neurostimulator) device was designed for rehabilitation of full spectrum other neurological symptoms in the most difficult conditions – chronic stages of TBI and Stroke. There is no feedback and no microcomputers inside. It is a device for brain stimulation. You can find more informations in the second Norman Doidge book, « The brain’s way of healing », chapter 7.
And at site Helius Medical Technologies:
http://www.heliusmedical.com/
PoNS is certified in Canada but not yet in USA – hopefully – end 2018. Before that – no one can buy or use it besides TBI patients, adults, in official clinical trials.
For example :
I think they will do study for mild TBI ( 20 participants)?
Kessler Institute for Rehabilitation?
I think they will start 30 November ?
https://clinicaltrials.gov/ct2/show/NCT03732755?term=PoNS&rank=1
The only chance to try it, and to test – is to travel to Moscow.
PoNS and CP was studed in Russia :
Here is information about CP clinic where they did clinical trail with Pons in Russia, Sankt Petersburg:
Contact:
Vestnik:
Publication in Russian:
(So just 1-2 November 2018 this cp study was presented to international Congress in Moscow ) hire translation and photos in Russian 🙂
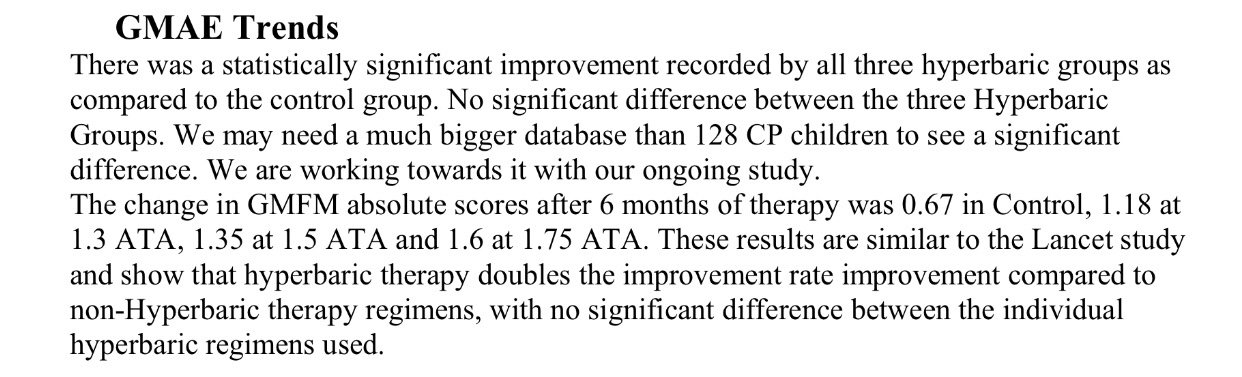
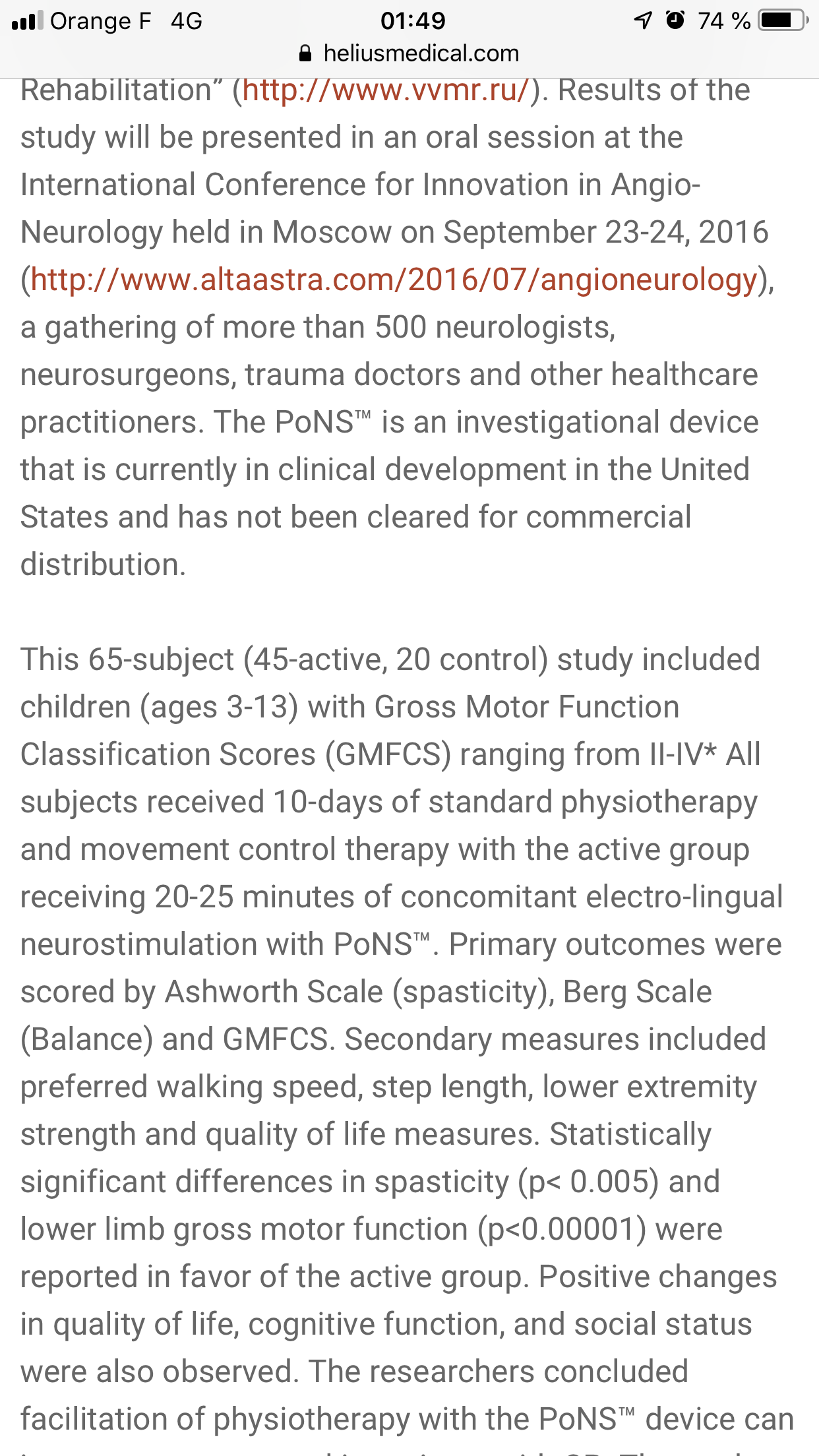
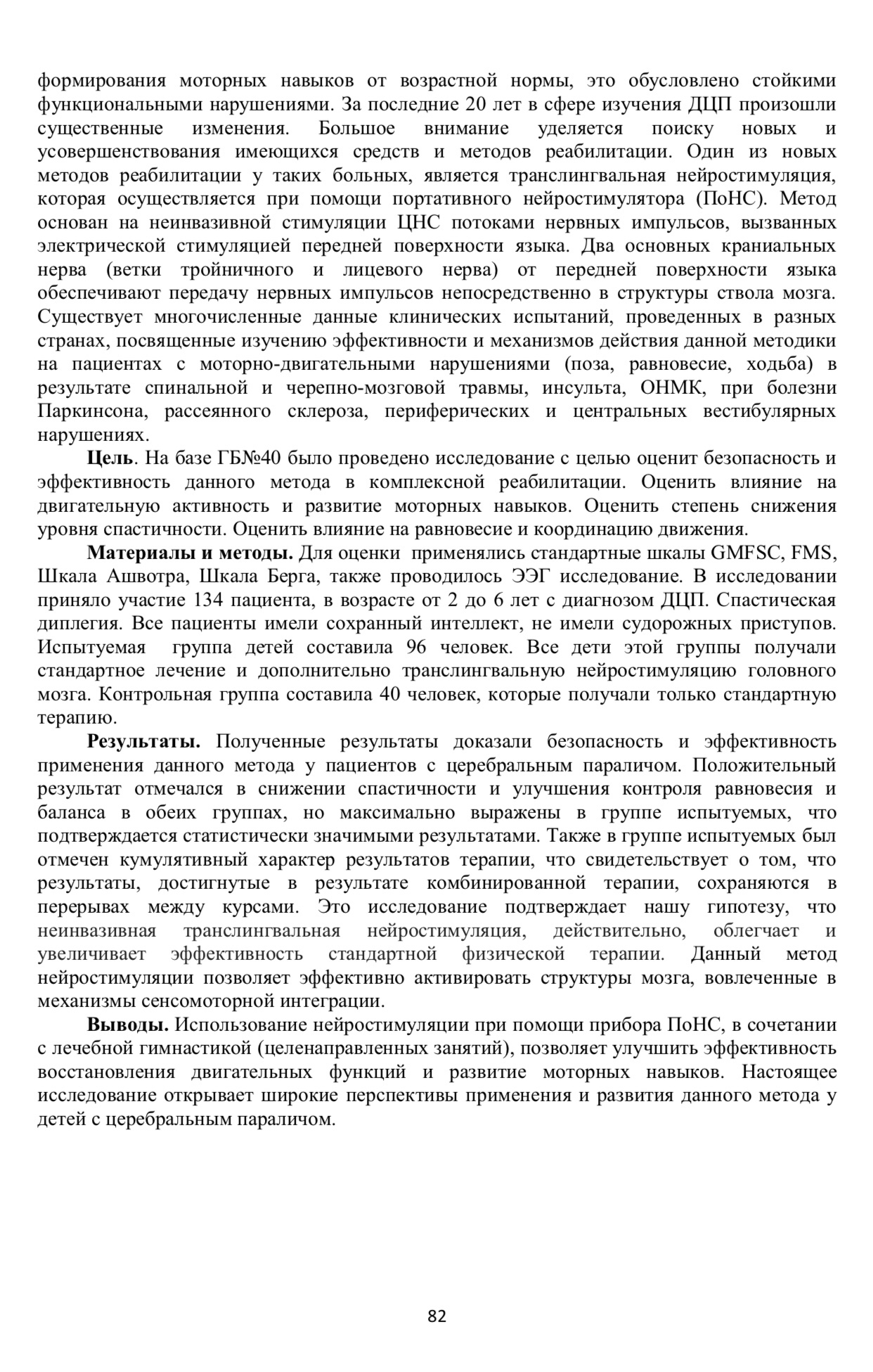
« Materials and methods. Standard scales GMFSC, FMS, Ashvotr Scale, Berg Scale were used for the evaluation, and an EEG study was also conducted. The study involved 134 patients, aged 2 to 6 years with a diagnosis of cerebral palsy. Spastic diplegia. All patients had intact intelligence, did not have convulsive seizures. The test group of children was 96 people. All children in this group received standard treatment and additionally translingual neurostimulation of the brain. The control group consisted of 40 people who received only standard therapy.
Results. The results obtained proved the safety and efficacy of this method in patients with cerebral palsy. A positive result was observed in reducing spasticity and improving balance and balance control in both groups, but was most pronounced in the group of subjects, as evidenced by statistically significant results. Also in the group of subjects, the cumulative nature of the results of therapy was noted, which indicates that the results achieved as a result of the combination therapy remain in the intervals between the courses. This study supports our hypothesis that non-invasive translingual neurostimulation is, indeed, facilitates and increases the effectiveness of standard physical therapy. This method of neurostimulation effectively activates the brain structures involved in the mechanisms of sensorimotor integration. Findings. The use of neurostimulation with the help of the PONS device, in combination with therapeutic gymnastics (targeted exercises), can improve the efficiency of the restoration of motor functions and the development of motor skills. This study opens up broad prospects for the use and development of this method in children with cerebral palsy. »
Source: http://association-dcp.ru/wp-content/uploads/2018/11/tezis_2018.pdf
Lecture Danilov nerorehabilitation:
PoNS in France:
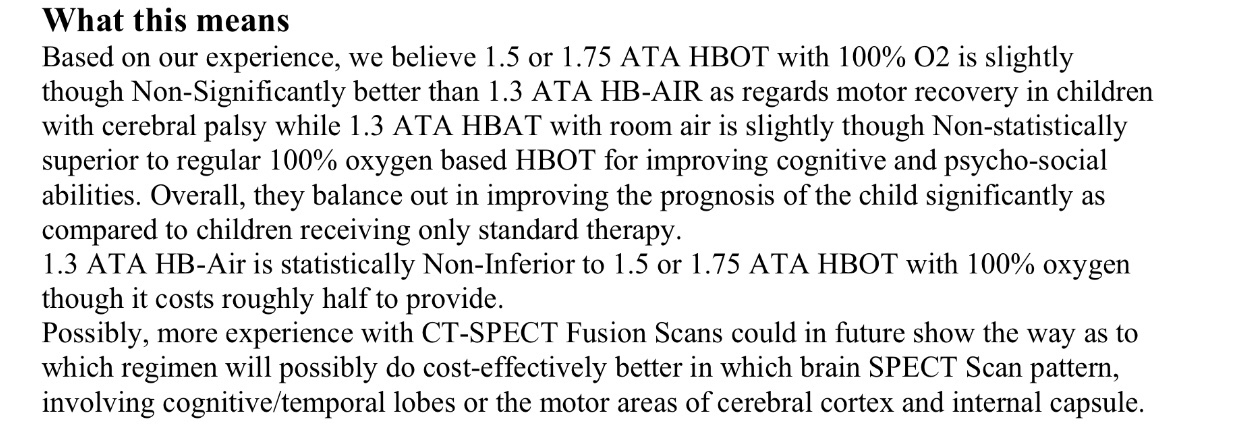
Helius Medical Technologies, Inc. Announces MRI Confirmatory Evidence of Neuroplastic Change after Investigational PoNS™ Treatment Presented at the 2018 Joint Annual Meeting ISMRM – ESMRMB in Paris, France:
« The main conventional approach for treating traumatic brain injury related gait and balance deficits has been through physical therapy, but few approaches have focused on brain based rehabilitation efforts that create direct neuroplastic changes. There remains a need for such an approach. Therefore, the goal of this study was: 1) to apply Cranial Nerve Non-Invasive NeuroModulation (CN-NINM) via the tongue in combination with multiple symptom-specific physical therapy exercises in patients with mild to moderate TBI, and 2) to investigate and quantify gray matter volume changes prior to and after intervention as well as their correlation with behavior. »
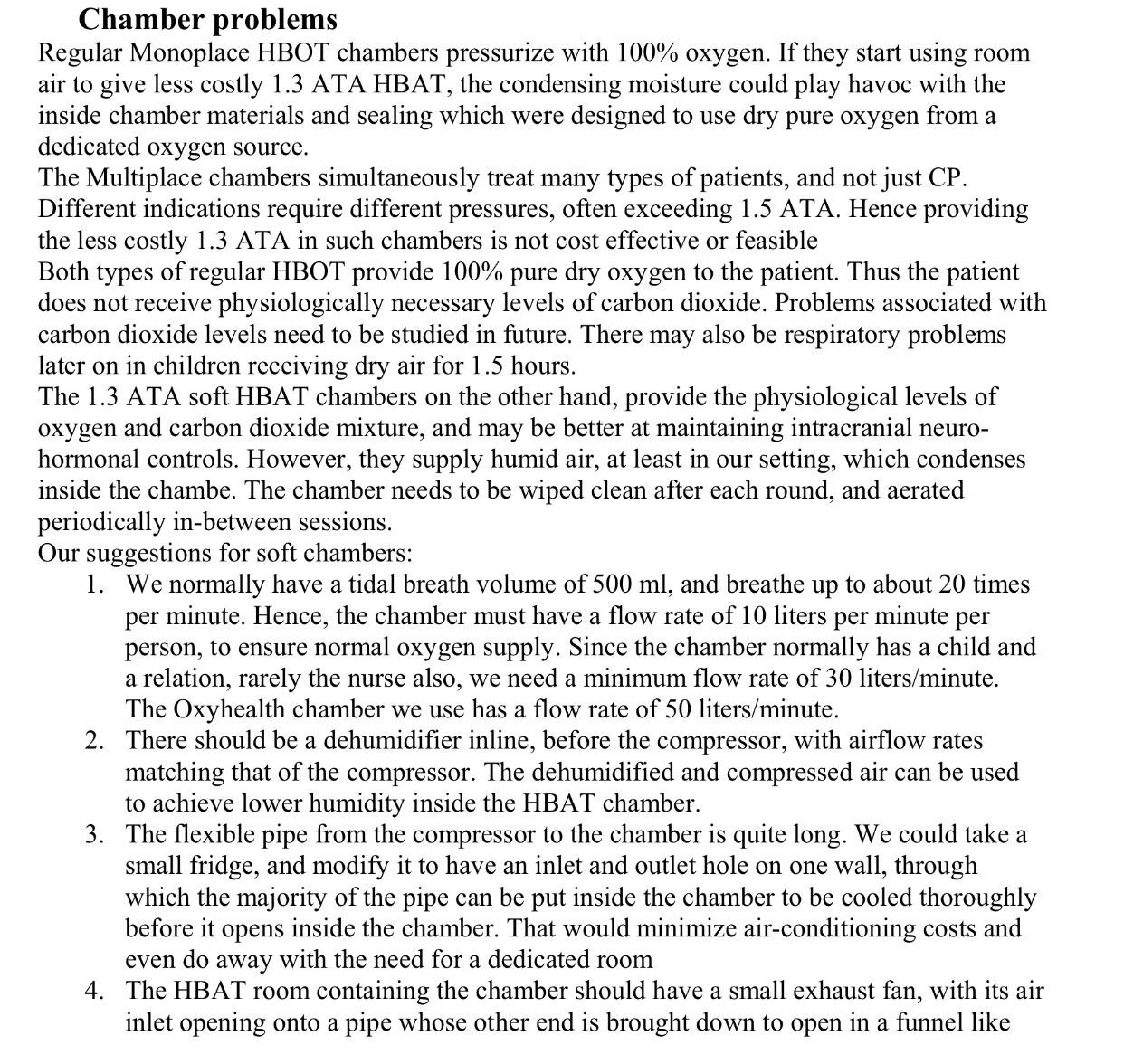
The PoNS™ device uses electrotactile waveform in conjunction with the Cranial Nerve – Non-Invasive NeuroModulation (CN-NINM) intervention. This involves using both balance and gait training methods to stabilize symptoms, regain balance & gait, and affect the functional transfer of improved stability and mobility to activities of daily living. It is based on a body of work focused on developing the tongue-based human-machine interface and application of this technology for balance, vision, and auditory substitution and more recently as neuromodulation for brain rehabilitation after injury and disease.
“143 electrodes and fits on the anterior portion of the tongue, to be held securely in place by the lips. The PoNS device uses an unbalanced biphasic waveform designed to ensure net zero current to reduce chance of tissue irritation, and has 19 V max and 6mA operational limits. Pulses are delivered to the tongue in triplets of pulses at 5 ms intervals every 20 ms. The subject can control the pulse-width (0.4-0.6 s) by adjusting the intensity buttons on the device.”
Read This study: for stroke patient:
More to read and watch about pons:
Fille cp
Premieres 10 minutes
De minute 26 (autres conditions neurologiques que MS)
Russian PhD dissertation written by Vadim Vladislavovich Deineko about the study:
Pons Canada :
info@neuromtl.com
Contact Mr Mazaltarim (Mazaltarim Marcel) at 514-481-7867
https://heuro.ca/
Heuro Canada, #201- 13737 96 Ave., Surrey, BC, V3V 0C6
(778) 819-1484
Maureen@heuro.ca
Or
https://neuromtl.com/
(Mazaltarim Marcel )
will have this soon. Stay tuned.
But Montreal indicated they will not be able treat patients with CP
Besides, even for diagnosis where they do offer treatment, minimum age is 18
Very disappointing indeed
Moscow pons: clinic is located 25 km from Moscow,
MOSCOW REGION, ISTRINSKY AREA, PAVLOVSKAYA SLOBODA, Lesnaya STR, 8
Bugorskiy Evgeny M
+7(495)2115170
medsyst@hotmail.com
Rehaline clinic,
25 km from Moscow, email above.
+7 (495) 211-51-70
rehaline@yandex.ru
ПН – ПТ с 9 до 18
Just some part for you from photo translation :
« Portable neurostimulator poNS allows you to restore the brain after diseases and injuries, as well as improve skills in a healthy person. The effectiveness of the technique has been proven in more than 5,000 patients with various neurological diseases of the last 10 years. Advantages of the method: non-invasive stimulation, no surgical insertion of electrodes, effects on the brain stem along natural pathways, restoration of function regardless of the initial cause of deterioration, a small number of relative contraindications, the effect of use in a wide age range. »
For contact and coordination, please send a letter to:
medsyst@hotmail.com,
Dr. Evgeny Bugorsky
Others devices :
About SYMPATHOCOR:
It’s an other device ( studed and invented in Russia): I honestly don’t know enoth about just wanted to mention it and so you can study yourself :
« The Simpatokor 01 apparatus, which puts these principles into practice, is included in the Russian StateRegister of Medical Devices (registration certificateNo. FSR
2007/00757 of September 28, 2007). Medicalmethods used in treatment with the Simpatokor 01 support stimulation of the cervical ganglia of the sympathetic trunk with the fields described above. The efficacy ofthis approach has been confirmed by results from theclinical use of the apparatus both at the prenosologicalstage and in the treatment of patients with migraine,autonomic vascular dystonia, hypertension (includingstable arterial hypertension resistant to standard therapy),the sequelae of closed craniocerebral traumas and cerebral concussion, hyperhidrosis syndrome, orthostatichypotension syndrome, and postural tachycardia,vestibulopathy syndrome, drug resistant epilepsy, neurosis syndromes, depression anxiety spectrum disorders, and attention deficit hyperactivity disorder, and alsofor the effective elimination of invasive units, recoveryfrom the state of alcohol and drug withdrawal, and forrestoration of auditory and visual functions ».
(PDF) New Principles for the Organization of Neurorehabilitation.
Hire study pons and SYMPATHOCOR together :
More:
Study in Russian about sympatocor :
BrainPort Balance device
« BrainPort Balance device is the sensory substitution device, using electrotactile neurofeedback to stabilize the subject head and it was originally designed to help people with peripheral vestibular disorders – to fix posture, body alignment and static balance control. See the Norman Doidge book – » Brain that change itself », chapter 1. It is still the best device for the purpose. «
Study with BrainPort :
Improving the Motor Skill
of Children With Posterior Fossa
Syndrome: A Case Series
The brainport was approved in Canada only. Not the USA
Pons ( немного информации по русски):
Разработан нейростимулятор языка для пациентов с двигательными нарушениями: Понс
Устройство стимулирует создание новых нервных путей в головном мозге, необходимых для восстановления двигательных функций при ДЦП, травмах, рассеянном склерозе и других заболеваниях.
Ученые из университета Висконсин-Мэдисон создали портативный нейромодуляционный стимулятор (Portable Neuromodulation Stimulator, PoNS), который позволяет воздействовать на головной мозг через язык человека.
При работе PoNS на протяжении 20-30 минут происходит неинвазивное нейромодуляционное воздействие на черепные нервы (cranial nerve non-invasive neuromodulation, CN-NiNM). Как показали эксперименты, при этом в мозге пациента образуются новые нервные связи. Это улучшает организационные способности мозга и запускает процессы восстановления контроля над нервной системой.
PoNS будет эффективным дополнением к основному курсу реабилитации людей, получивших черепно-мозговую травму, переживших инсульт, а также страдающих от детского церебрального паралича (ДЦП), болезни Паркинсона или множественного рассеянного склероза. ( почитайте книгу Нормана доджа).
Исследование сделанное в Питере для детей с дцп:
ВЛИЯНИЕ ТРАНСЛИНГВАЛЬНОЙ НЕЙРОСТИМУЛЯЦИИ ГОЛОВНОГО МОЗГА НА ФОРМИРОВАНИЕ МОТОРНЫХ НАВЫКОВ У ДЕТЕЙ
С ЦЕРЕБРАЛЬНЫМ ПАРАЛИЧОМ
Игнатова Т.С.1, Скоромец А.П.2, Колбин В.Е.1,Сарана А.М.1,3, Щербак С.Г.1,3, Данилов Ю.П.4
:
Материалы и методы.
Для оценки применялись стандартные шкалы GMFSC, FMS, Шкала Ашвотра, Шкала Берга, также проводилось ЭЭГ исследование. В исследовании приняло участие 134 пациента, в возрасте от 2 до 6 лет с диагнозом ДЦП. Спастическая диплегия. Все пациенты имели сохранный интеллект, не имели судорожных приступов. Испытуемая группа детей составила 96 человек. Все дети этой группы получали стандартное лечение и дополнительно транслингвальную нейростимуляцию головного мозга. Контрольная группа составила 40 человек, которые получали только стандартную терапию.
Результаты. Полученные результаты доказали безопасность и эффективность применения данного метода у пациентов с церебральным параличом. Положительный результат отмечался в снижении спастичности и улучшения контроля равновесия и баланса в обеих группах, но максимально выражены в группе испытуемых, что подтверждается статистически значимыми результатами. Также в группе испытуемых был отмечен кумулятивный характер результатов терапии, что свидетельствует о том, что результаты, достигнутые в результате комбинированной терапии, сохраняются в перерывах между курсами. Это исследование подтверждает нашу гипотезу, что неинвазивная транслингвальная нейростимуляция, действительно, облегчает и увеличивает эффективность стандартной физической терапии. Данный метод нейростимуляции позволяет эффективно активировать структуры мозга, вовлеченные в механизмы сенсомоторной интеграции.
Выводы. Использование нейростимуляции при помощи прибора ПоНС, в сочетании с лечебной гимнастикой (целенаправленных занятий), позволяет улучшить эффективность восстановления двигательных функций и развитие моторных навыков. Настоящее исследование открывает широкие перспективы применения и развития данного метода у детей с церебральным параличом.
http://association-dcp.ru/wp-content/uploads/2018/11/tezis_2018.pdf
( осторожно в России так же продают теперь подделку!!!!)
Нейропорт – криво сделанная самоделка имитирующая ПоНС, с неправильными сигналами, опасная в применении.
Не покупайте это!