
( I will say study wich makes people argue)….
Will be 1,3 ata without oxygen enough for CP?
Or 1,5ata with 100% oxygen is better ???
This is the question ! Is only one study enoth to answer it? I don’t know….
Are all children’s with CP need same protocol ?
🙂
here the study comparing 1,3 ata air
With 1,5ata
With 1,75 ata
( it was published by Dr Arun Mukerjee India):
Please see his conclusions :
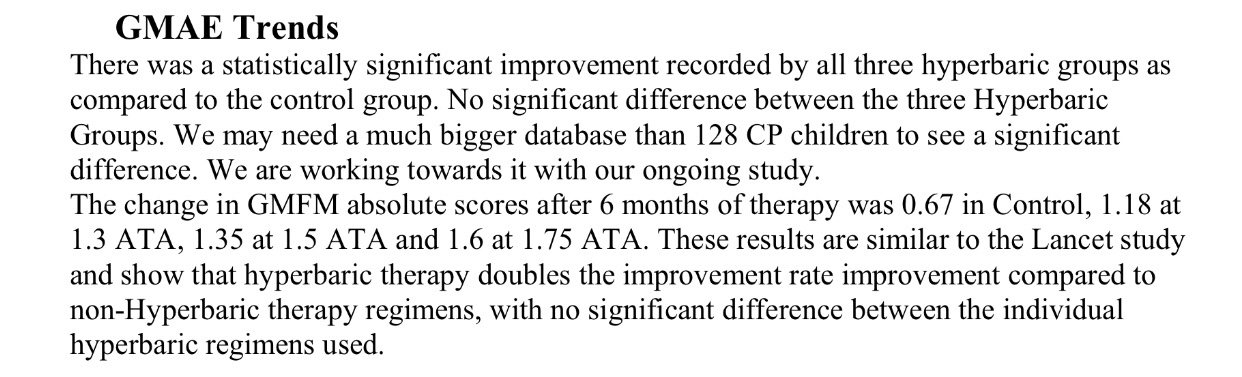
So in fact conclusion is that all Hbot groups give improvements with no significant differences …. and that more study neded….
An this study was made in India with help of dr Marois (Canada)…..
In fact, this study compares the use of various hyperbaric pressures with the use of (ambient) air alone or oxygen-enrichment in the treatment of children with Cerebral Palsy (CP). The study shows that low pressure ambient air hyperbaric therapy (1.3 atmospheres-ATA) is also effective not only high pressure 100% oxygen (1.5 or 1.75 ATA) in the treatment of CP.
The children were studied by Dr. Arun Mukherjee, director of the UDAAN Disabled Children’s Center, a non-profit organization, recognized and aided by the Indian Ministry of Social Justice & Empowerment.
This landmark study, co-authored with Dr. Pierre Marois (McGill University in Montreal, Canada), further develops the 1999 ground-breaking McGill study (Lancet, February 2001) by expanding the number of subjects and by implementing an accurate placebo-control testing method. Subjects with a functional diagnosis of spastic diplegia cerebral palsy received one of four hyperbaric options, in addition to standard therapies:
1) the placebo therapy (20 subjects);
2) hyperbaric therapy at 1.3 ATA breathing ambient air under pressure (36 subjects);
3) hyperbaric therapy breathing 100% oxygen at 1.5 ATA (32 subjects); and
4 ) 1.75 ATA with 100% oxygen (58). All subjects were reevaluated at six months after conclusion of therapy to negate any traces of the placebo effect.
The study showed significant improvements FOR ALL THREE GROUPS receiving therapy hbot !!!!!(the placebo group showed little or no improvement).
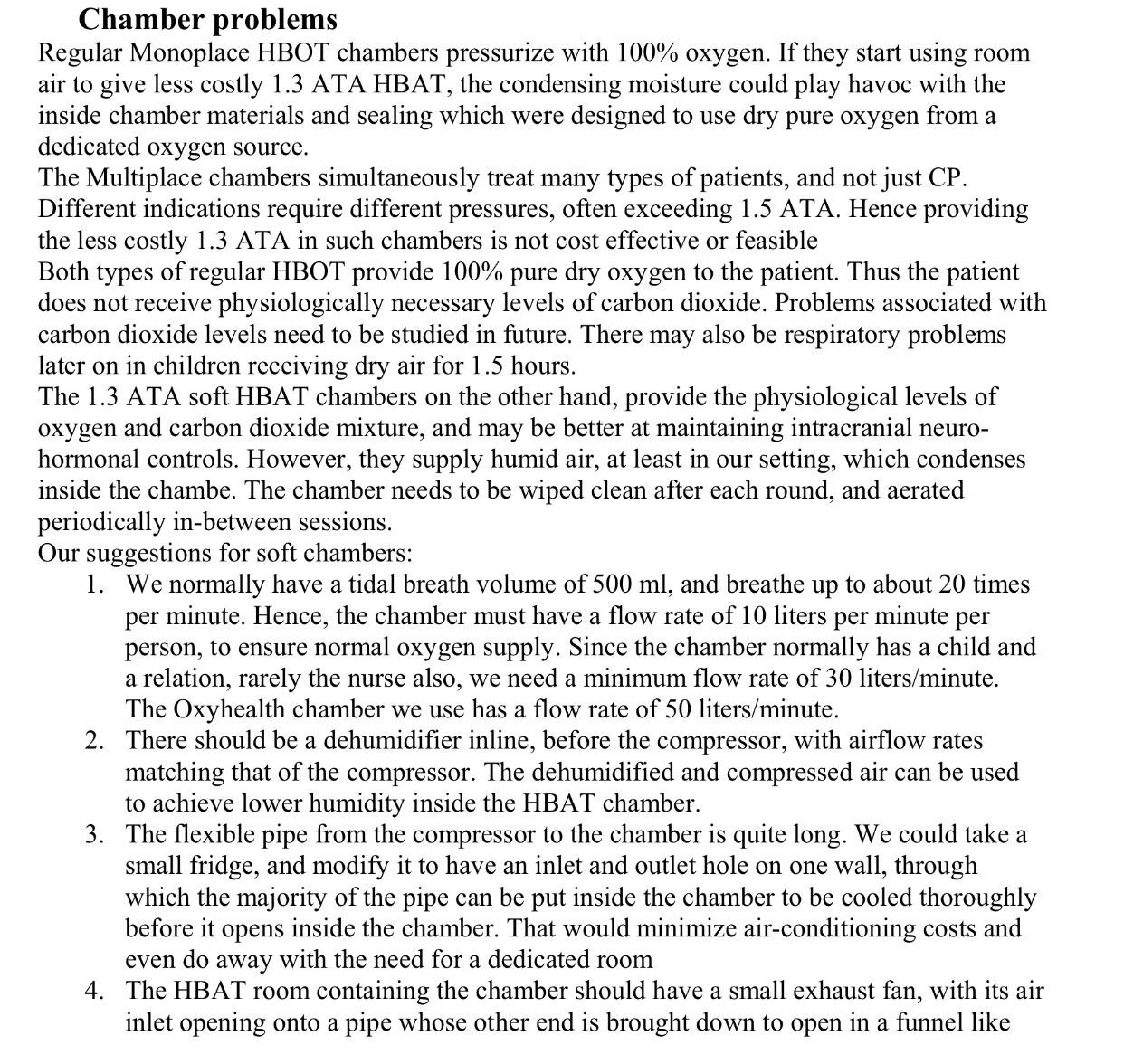
They mentioned in study that 1,3 ata could be an option for parents who can’t afford 1,5 ata to get far degree of improuvments (read also please paragraph about chambers problems…)
They also mentioned in study:
…..”it is possible that the cp child with greater motor dysfunction will be slightly better with regular hbot 1,5 ata 100% oxygen”
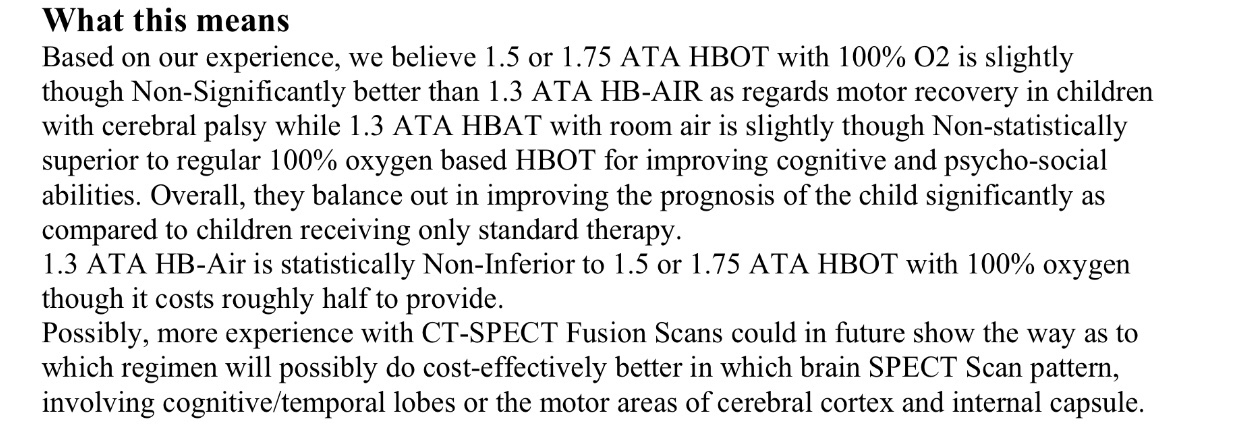
So we need more studies to be shure which pressure is better for cp … in meantime wile we have no such studies I will be happy if parents with CP child trying any law neurological pressure …( better with Hbot doctor guidence ) so any law pressure 1,3 or 1,5 or 1,75 ….
Read all study… in details and do best you can for your children’s 😉
Bottom line ( pressure) is nobody really knows yet which is the best protocol.
Weakness if this study: absence of spect scans for all 3 groups with Hbot treatments before treatment and after.
As dr Efrati said in his research: « Unfortunately, in many – if not most – clinical studies done with hyperbaric oxygen on brain-in- jured patients, including those with cerebral palsy, the stunned areas have not been assessed by imaging. The anatomical/physiological imaging should be incorpor- ated as an essential part of the basic evaluation of every candidate for hyperbaric oxygen therapy. »
This study in India was done without any spect or MRI ….
But what firsthand we have to think when we talk about brain injury and CP: obviously more studies are needed!
And i think parents can help in someway to push for Hbot if we contact enough gouvernements / researchers/ media’s we need to take Hbot in the “light “ in order that general population knows about and that Hbot can help neurological conditions we need work all together not in separate camps… 😉 and doctors have to stop taking -us – parents like we are absolutely stupid 😉
( unfortunately we have some doctors which thinks we can only listen their orders) we are also need to study ( parents) and we can also bring some informations to doctors if they wants to listen us 😉
“Clearly, large-scale, well-controlled, pressure dose- response studies are required to determine the optimal HBO2 therapy protocol for different conditions. Until such information is available, any treatment involving change in the environmental pressure should be con- sidered as a dose-comparison rather than a sham-control study. Moreover, since at a young age, brain protection is stronger (reflected by high ROS levels associated with CP) and neuroplasticity is more potent, it is reasonable to expect that optimal efficacy will be achieved by lower tissue oxygenation. Along such line of reasoning, the previously described trials used 2.0 atm abs for post- stroke patients and 1.5 atm abs for patient with mTBI with an intact macrovascular bed [23,24]. Due to the high diversity in the manifestation of cerebral palsy and in its severity, future efforts should also be directed towards a personalized dose-response curve. For example, it is likely that higher tissue oxygenation will be the practice of choice for children with a high expression of ApoE4, which is an inhibitor of mitochondrial respiration.”
And : “One must bear in mind that children with CP suffer neurological deficiency since birth, so it will take time for the brain repair to become clinically apparent. For example, it is not reasonable to administer 20 daily HBO2 sessions to children with pervasive developmental disorders (PDD) and expect to see significant clinical progress within a time frame of less than a month [25].
On the other hand, it is important to perform fre- quent metabolic/physiological evaluations, which may provide valuable information for adjusting the dose- response curve. More studies are needed to determine the minimal effective dosage and the treatment duration for specific brain injuries. Non-invasive, in-chamber measurements that are currently being developed, speci- fically EEG and DTI, may shed some light on this important question.”
And: “the optimal candidate for hyperbaric oxygen is a patient with unrecovered brain injury where tissue hypoxia is the limiting factor for the regeneration processes. In this patient, HBO2 may induce neuroplasticity in the stunned regions where there is a brain anatomy/physiology (e.g., SPECT/CT) mismatch [23,”
Source: