Bonjour j’ai posté ça avant par morceaux mais ici je donne plus informations :
Déjà comeser lire cet étude au moins bien expliqué en français pour Hyperbare et IMC:
« Malgré la controverse à propos des résultats, l’étude de Collet et al. (2001) a ouvert la voie à d’autres recherches au sujet de l’OTH pour la PC. La question de savoir ce qui a produit des améliorations chez les participants demande une réponse. Il serait certainement bénéfique de répéter cette étude, cette fois en incluant un groupe avec 100 % d’oxygène pressurisé, un groupe avec de l’air pressurisé à 1,3 ATA, un groupe avec 27 % d’O2 à 1 ATA et un groupe avec de l’air non pressurisé, ce dernier servant de vrai groupe contrôle. Ces résultats pourraient même démontrer que l’OTH tel que défini par la UHMS en 2006 (Undersea and Hyperbaric Medical Society, 2007) (100 % d’O2 à un minimum de 1,4 ATA) n’est pas nécessaire pour traiter les enfants avec la PC si un traitement atténué, avec de l’air légèrement pressurisé (21 % d’O2 à 1,3 ATA) ou même avec 27 % O2 à 1 ATA, peut faire le travail.
Jusqu’à tout récemment, la position du gouvernement québécois n’était pas vraiment favorable à toute recherche additionnelle sur les effets de ce traitement sur les enfants atteints de PC. En s’en tenant à cette position, il s’est aligné avec laposition adoptée par Santé Canada en 2006, qui reconnaît l’efficacité de l’OTH pour le traitement de certaines conditions, mais contredit formellement son efficacité pour la PC, en mentionnant que : « à l’heure actuelle, rien ne supporte l’utilité de ce traitement (Santé Canada, 2006)». Néanmoins, une loi adoptée en mars 2005 autorise le ministère du Revenu du Québec à accorder des crédits d’impôts aux familles québécoises pour traiter les enfants atteints de PC à l’aide de l’OTH (Pineau, Maqadem, 2007). De plus, en mai 2006, le ministère de la Santé du Québec a confié à l’Agence d’évaluation des technologies et des modes d’intervention en santé (AETMIS) le mandat d’évaluer l’efficacité de l’OTH pour la PC (Gouvernement du Québec, 2005). Le rapport de l’AETMIS concluait qu’il y a suffisamment de preuves pour recommander d’autres recherches sur les effets de l’OTH pour la PC.
Plusieurs questions ont besoin d’être abordées, dont l’effet de la participation à une recherche organisée, la pression optimale ou minimale et la concentration d’oxygène nécessaires, ainsi que la quantité et la fréquence des traitements requis pour produire un résultat maximal. »
https://www.researchgate.net/profile/Serge_Larivee2/publication/317588283_L%27oxygenotherapie_hyperbare_dans_le_traitement_de_la_paralysie_cerebrale_arnaque_ou_traitement_approprie/links/59418e950f7e9b1d452de236/Loxygenotherapie-hyperbare-dans-le-traitement-de-la-paralysie-cerebrale-arnaque-ou-traitement-approprie.pdf?origin=publication_detail

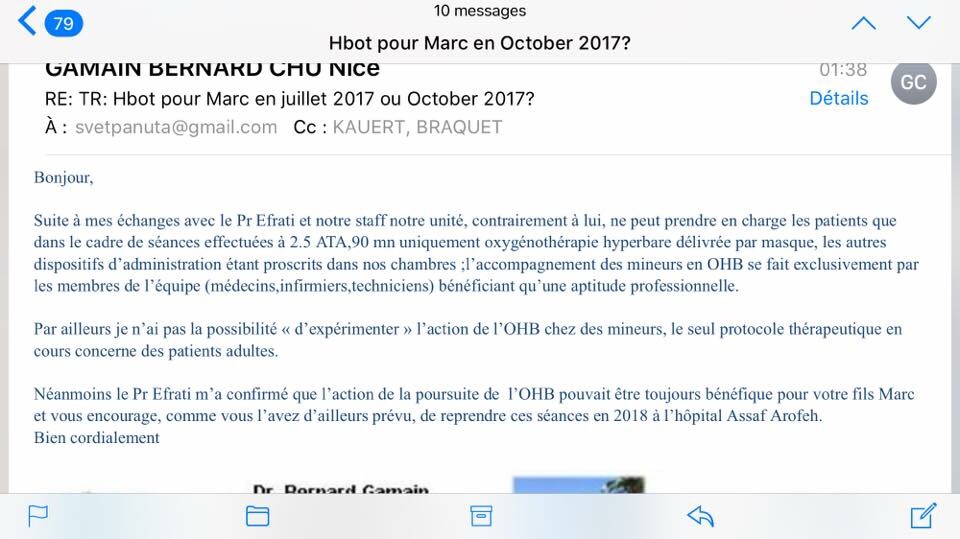
Réponse de Dr Gamain (Hbot à Nice qui fait en france etude pour les adultes ) Mais visiblement c’est pas encore administrativement possible pour enfants ;( en hôpitaux
Pauvre enfants français …..
article sur étude faite en France pour les adultes ( dr Gamain( Chu Nice)
Émission de 22 octobre 2018: « allo docteurs »
Au moins il parle de hbot en france ( pour adultes après avc à Nice et interview avec dr Gamain) ….regarder après minutes 15…..
https://mobile.france.tv/france-5/allo-docteurs/756463-allo-docteurs.html
Si ce lien marche pas vous pouvez regarder extrat ici:
https://youtu.be/nHMMH3d7hiM
j’ai l’espoir que ça va changer un jour 😉 enfin nous avons Dr Gamain (Nice) la il fait des études officielles pour les patients adultes AVC et en France nous avons seulement Hbot dans les hôpitaux (Médecine sociale) donc j’espère que Plus tard, il fera étude pilote pour les enfants??? en tout cas je lui a envoiee toutes les données Marc ainsi que j’ai discuté avec lui par téléphone de ce qu’il a fait (il était très honnête avec moi, il a dit qu’en France il ne peut pas avec des enfants mais il m’a conseillé de repartir à Israël et de faire ( encore un peut plus Hbot)



Mais!
Dans cet article je vous donne tout informations à ma connaissance sur Hyperbare en france ( quel est biensure pas encore reconnu pour IMC…mais honetment quends je vois tout les témoignages à l’international …. çà fait réfléchir)…..
Parents Canadiens se batte pour la faire reconnaître et rembourser caisson hyperbare pour enfants IMC:
L’Institut national d’excellence en santé et en services sociaux (INESSS) s’est vu confier le mandat d’évaluer la valeur thérapeutique de l’oxygénothérapie hyperbare dans la prise en charge de la paralysie cérébrale. J’espère ils vont réussir….
Vous pouvez voir sur lien:
https://fr.surveymonkey.com/r/Appel_OHB?fbclid=IwAR1NSh_IHT1x4H1lbECr0noohwUMC9Odl2xMm-EvBe9jbYy9kRuIpinL1AQ
En 2014, le Dr Marois fut coauteur d’une étude historique sur l’OHB administrée à diverses pressions qui portait sur 150 enfants indiens atteints de paralysie cérébrale. Cette étude confirma ce qu’il observe chez ses patients depuis 20 ans (voir ces reportages de Télé-Québec et des Nouvelles TVA). Après avoir fait 40 sessions d’OHB d’une durée de 60 minutes, 120 enfants ont connu trois fois plus de progrès de leurs fonctions motrices et cérébrales que ceux du groupe contrôle ayant reçu d’autres traitements physiques. Fait important à noter, les améliorations étaient remarquables pour toutes les pression (1,3, 1,5 ou 1,75 ATA) et la concentration d’oxygène (21 ou 100 %) administrées.
Le Dr Marois conteste l’évaluation que fait le gouvernement du Québec de l’OHB basse pression. « Des considérations politiques et économiques, plutôt que purement scientifiques, jouent un rôle important dans cette controverse. D’autres recherches systématiques sont requises, mais entre temps les enfants ne devraient pas se faire refuser l’accès à » l’OHB », écrivait-il avec des collègues en 2007 dans le Journal of American Physicians and Surgeons.
L’étude qu’il a cosignée en 2014 fut la toute première au monde à démontrer que l’OHB basse pression (1,3 à 1,75 ATA) améliore les fonctions motrices et cérébrales d’enfants atteints de paralysie cérébrale. « Alors qu’ils étaient presque tous en fauteuil roulant, plusieurs d’entre eux ont recommencé à se déplacer », a-t-il expliqué le 6 mars 2014 à l’émission Une pilule, une petite granule, de Télé-Québec. « En élevant les niveaux d’oxygène dans le cerveau, les traitements hyperbares permettent de remettre en marche des cellules qui n’avaient pas été détruites mais qui avaient été secouées par la lésion initiale au point de se retrouver en état d’inertie, précisait le physiatre dans Le Devoir du 10 avril 2014. Ils stimulent la circulation sanguine dans le cerveau et la création de nouveaux vaisseaux. Ils accroissent le métabolisme cellulaire. Ils augmentent le nombre de cellules souches circulant dans le cerveau. Ils réactivent les cellules réparatrices ainsi que les mécanismes de réparation cellulaire. »
https://maisonsaine.ca/wp-content/uploads/2017/12/hbot-cp-and-edito-uhms-2014.pdf
Cette étude se voulait une réponse à une étude commandée par le gouvernement du Québec et publiée dans la prestigieuse revue médicale The Lancet, en février 2001. Son auteur, le Dr Jean-Paul Collet, de l’Hôpital Général Juif de Montréal, avait conclu que les améliorations observées chez des enfants atteints de paralysie cérébrale, ayant reçu 100 % d’oxygène à 1,75 ATA, étaient les mêmes que celles d’un groupe dit « placebo » recevant de l’air (donc 21 % d’oxygène) à 1,3 ATA, pression qui selon le Dr Collet serait sans effet, rapportait alors l’Agence Science Presse. Le Dr Marois conteste cette interprétation reprise par le Fonds de recherche en santé du Québec (FRSQ) qui répète depuis des années cette affirmation qu’il qualifie de désinformation. En effet, il rappelle que les sacs Gamow, qui appliquent une pression de 1,3 ATA pour traiter les grimpeurs malades en haute altitude, sauvent des vies chaque année. Une étude de Collet et al. a d’ailleurs mesuré et attesté les bienfaits d’une petite augmentation de pression, même sans ajout d’oxygène supplémentaire.
Comme le Dr Marois l’affirmait en 2002 dans le cadre du Congrès international sur la médecine hyperbare, tenu à San Francisco [notre traduction] : « L’oxygénothérapie hyperbare à 1,3 ATA [atmosphère ou bar] n’est en aucun cas un traitement placebo, les effets de l’augmentation de la pression augmente également la quantité d’oxygène dissous dans le tissu corporel de plus de 50 %. Il y a de plus en plus de preuves qui démontrent que le traitement hyperbare à basse pression induit des changements permanents dans un cerveau endommagé. Les études du Dr Heuser à U.C.L.A. et des expériences avec des milliers de cas en Russie, ainsi que certaines études chez l’homme et le rat, suggèrent que l’OHB même à une pression aussi faible que 1,1 ATA est efficace pour améliorer les compétences fonctionnelles et l’imagerie par balayage SPECT. »
Vous pouvez trouver article sur
Claudine Lanoix ( pioneer Hyperbare du Canada pours ses enfants IMC) :
http://brain-injury-hope.com/2019/01/claudine-lanoix-story-and-hbot/
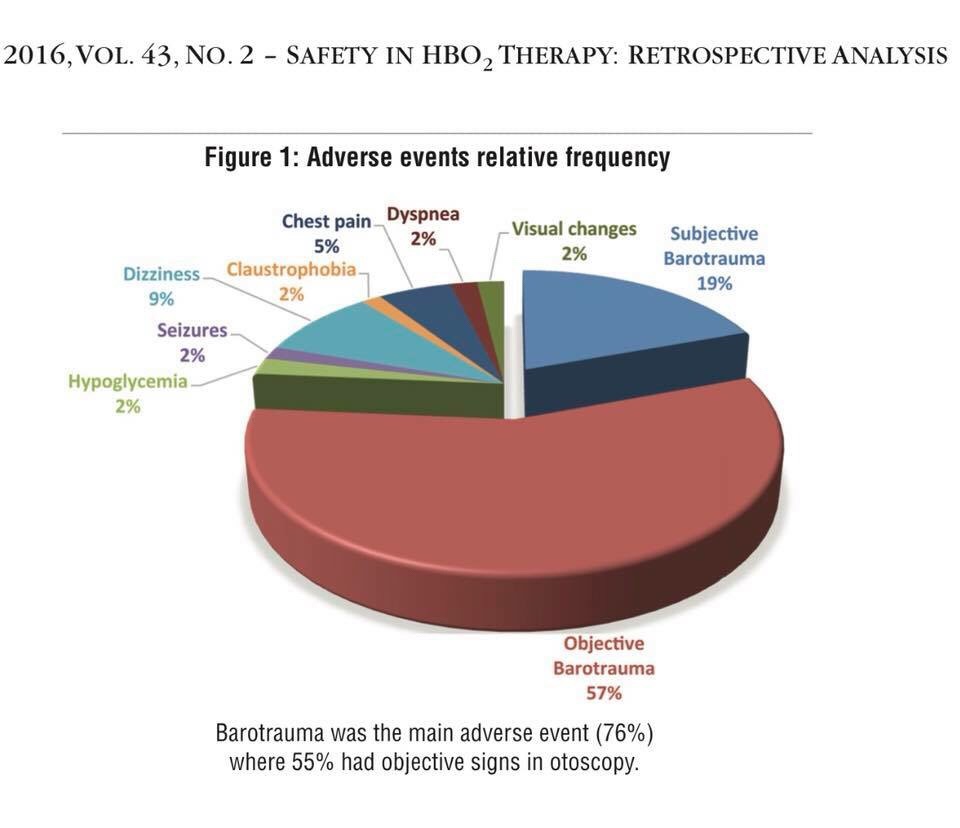
Claudine Lanoix qui a fondé le Centre hyperbare de l’île, à Pincourt, avec son mari Thomas Fox en 2004. Seule clinique privée en son genre au Québec, elle utilise des caissons rigides dont la pression varie entre 1,75 et 2,5 bar. Elle affirme que plusieurs personnes qui ont acheté ou loué un caisson souple de certains fournisseurs l’appellent pour de l’aide. « Les gens qui les utilisent à la maison ne sont pas toujours bien informés. Certaines personnes passent trop de temps dans la chambre hyperbare. Trop d’une bonne chose n’est pas bon », dit-elle en rappelant que l’oxygène est un oxydant qui génère des radicaux libres qui sont nécessaires mais pas en trop grande quantité. La principale plainte concerne les barotraumatismes. « Ils ont des blessures aux oreilles. Ils ont monté la pression trop rapidement et se sont blessé les oreilles. Si les gens sont congestionnés, il faut y aller doucement et leur montrer à déboucher leurs oreilles », en pinçant leurs narines et en soufflant.
La thérapie d’oxygène hyperbarique n’est pas sûre pour tous. En général, vous ne devriez pas la recevoir si vous avez certains types de maladies pulmonaires, à cause du risque d’affaissement pulmonaire, si vous avez un poumon affaissé, avez un rhume ou de la fièvre, avez récemment subi une chirurgie ou une blessure à l’oreille et n’aimez pas les petits espaces clos. »
Claudine Lanoix et Thomas Fox ont découvert cette thérapie en 1997 en cherchant à soigner ses deux fils atteints de paralysie cérébrale. Comme il n’existait alors aucune clinique hyperbare au Canada, ils ont suivi leurs traitements en Écosse, en 1998. « Nos enfants furent les premiers au Canada traités pour des blessures neurologiques avec l’OHB, raconte Mme Lanoix. L’un d’eux a alors commencé à marcher et l’autre a commencé à parler et à se redresser dans son fauteuil roulant. »
Formée en OBH à l’Université McGill et avec les sommités internationales dont le Dr Neubauer, Philip James et Paul Harch, elle avoue ne pas être familière avec les chambres hyperbares à basse pression. Elle explique que la haute pression — à partir de 1,75 bar — réduit la spasticité et est particulièrement indiquée pour les plaies parce qu’elle détruit plus efficacement les bactéries. « Les études sur les blessures sportives et les plaies utilisaient une pression de 2 à 2,5 ATA et 100 % d’oxygène car la pression supérieure le pousse plus profondément dans les tissus. Mais il y a indéniablement de la place pour les deux types de chambres.
Tout le monde devrait avoir accès à cette thérapie en centre de réadaptation. C’est vraiment triste que le gouvernements ne l’offre pas gratuitement par tout dans le monde…..
Pour instant en france Hyperbare est possible que en privé ( pas reconnu c’est souvent les parents qui prends décision et qui paye de leur poche)…..
Ou dernière information que j’ai pu avoir:
C’est bien le médecin de Nantes qui mène un programme de recherche. Des groupes d’enfants en ont bénéficié ces derniers mois. Il veut publier les résultats pour que cette thérapie soit reconnue officiellement et que les enfants y aient accès en France.
Apparemment que le pédiatre Guy Letellier à Nantes ( En France) est connaisseur et ouvert sur le sujet de Hyperbare.
Dr Guy LETELLIER, Secrétaire de la SFRP
Service de Médecine physique et réadaptation pédiatrique, SSR pédiatrique
ESEAN – Etablissement de Santé pour Enfants et Adolescents de la région Nantais
en privé:
Il y a deja 3 centres Hyperbare « Biobarcia « en france en faite ( privées) et ils vont ouvrir encore 2!
Et aussi :
Et il y’a possibilité de faire louer à Paris hbot souple:
OXYSOINS

Romy Guez sera responsable de cet option à mis en disposition par companie québécois :
https://oxysoins.com/
OxySoins un des références très connue concernant les séances en chambre hyperbare basse pression au Québec. ( chambres hyperbare souples) Que ce soit pour de l’information sur les chambre hyperbare, sur la location d’un caisson hyperbare à domicile, l’achat de l’appareil ou pour une session supervisée au Centre Hyperbare OxySoins.
Vous pouvez déjà communiquer avec
Romy Guez pour centre à Paris
via mail
paris@oxysoins.com ou par
téléphone au 01 86 65 56 85
maintenant Informations /contacts pour centres Biobarcia:

1. ouvert septembre dernière à Marseille) centre privé ostéopathe et qui propose Hyperbare :
Caisson souple « CE médical »
1,45 ata
92% +/-3%
Ici le lien:
https://oxyclair.com/
2. hbot il y a encore une en Var ( même type chambre même distributeur que à Marseille)
Les coordonnées du centre de Saint Raphael (Var)
Centre d’Oxygénothérapie Hyperbare
Place Pierre Coulet
Immeuble le St Louis
83700 Saint Raphael
Tel : 0628201626
mail : oxy.st.raphael@lienqualite.fr
Et
de l’ouverture de deux nouveaux centres d’Oxygénothérapie Hyperbare 1,45ata :
- 2 dispositifs à Nancy au sein de :
Médical Move Center
19 rue Blaise Pascal
54320 Maxéville
Tel : 06 12 03 93 86
Oxy.nancy@lienqualite.fr
- 1 dispositif à Lyon au sein de :
Centre de Médecine du Sport de Gerland
Avec l’équipe de Cryo-Advance
6 Avenue du Château Gerland, 69007 Lyon
Tel : 06 72 07 14 22
Et ici contact
distributeur de ce Dispositif Médical
Lionel DEBOULLE
Portable 06 52 03 40 12
Mail : info@lienqualité.fr
Site : https://www.lienqualite.fr
http://www.oxfordmedicaleducation.com/prescribing/oxygen-delivery/
J’espère un jour HBOT pour maladies neurologiques en France sera aussi accessible comme en Israël…..
Il y a beaucoup de patients pédiatriques en France qui présentent des séquelles d’accidents neuro vasculaires ou lésions cérébrales apres accidents: (noyade ou manque oxygène en raisons différentes) avec une qualité de vie altérée.. et le caisson hyperbare n’est malheureusement pas très connu ou pire mal reconnu en France.
Et ce, alors même que nous soyons très bien équipés en France en caissons hyperbares. Ceux-ci ne sont utilisés que pour la décompression ou pour l’intoxication au CO2 ou autres maladies (sur liste de remboursement de secu)….contrairement aux autres pays tels que les USA, Israël, la Chine ou l’Angleterre qui y soignent également les enfants avec lésions cérébrales, et où on peut trouver médecins qui font études pour victimes d’un AVC ou avec traumatismes crâniens. ( Dr. Efrati à Israël ou dr Harch à USA…)
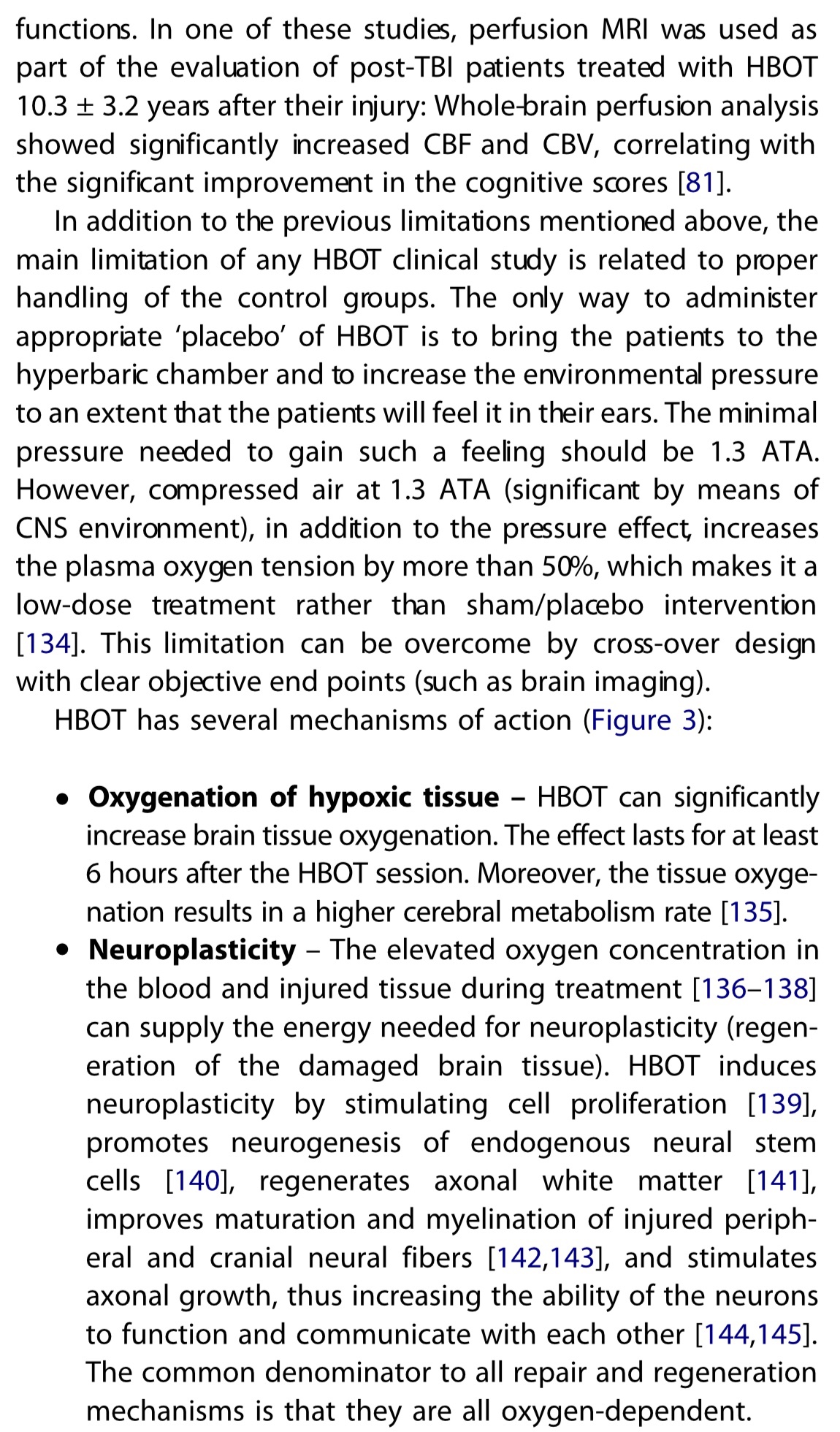
UNE ÉQUIPE DE CHERCHEURS EN NEUROSCIENCES DE L’UNIVERSITÉ DE TEL AVIV A DÉMONTRER L’INTÉRÊT DE L’ OXYGÉNOTHÉRAPIE (HYPERBARE), POUR LE CERVEAU DES TRAUMATISÉS CRÂNIENS. Traitement généralement utilisée pour les plongeurs victimes d’accidents de décompression, « Ces résultats démontrent que la neuroplasticité peut être activée des mois et des années après la lésion cérébrale », poursuit le spécialiste. Après un choc violent à la tête, le processus de régénération met en jeu des mécanismes complexes puisqu’il faut recréer des vaisseaux sanguins et des connexions entre les neurones. Or, ce type de mécanismes demande beaucoup d’énergie à l’organisme. « C’est en cela que l’oxygénothérapie hyperbare peut aider. Les niveaux élevés d’oxygène pendant le traitement apportent l’énergie nécessaire pour faciliter le processus de guérison », explique le Dr Shai Efrati, autre auteur de l’étude.
Pour cette étude, publiée dans la revue PLoS ONE, les scientifiques ont recruté 56 personnes, victimes d’un traumatisme crânien modéré au cours des 5 années précédentes et souffrant encore de séquelles telles que des migraines, des difficultés de concentration ou de mémorisation ou des troubles de l’humeur. Pendant deux mois, la moitié d’entre eux ont suivi 40 séances d’une heure en caisson hyperbare, respirant de l’oxygène pur à la pression équivalente à une plongée à 5m de profondeur, tandis que le groupe des témoins ne recevait aucun traitement pendant les 2 premiers mois puis la même série de 40 séances d’oxygénothérapie pendant les 2 mois suivants.
L’oxygène aide le cerveau à récupérer
Résultats ? Qu’elle soit immédiate ou décalée de 2 mois, la période d’oxygénothérapie a permis d’améliorer significativement la qualité de vie des patients et leurs résultats aux tests de fonction cognitive, notamment en matière de mémoire. Un contrôle par imagerie cérébrale (par TEMP ou tomographie d’émission monophonique) a également montré une activité accrue des neurones après le passage en caisson hyperbare.
« Ce qui rend ces résultats encore plus convaincants, c’est la concordance remarquable entre la restauration des fonctions cognitives et les modifications de la fonctionnalité du cerveau détectées grâce à l’imagerie », souligne l’un des auteurs, le Pr Eshel Ben-Jacob.
Ici étude ( en anglais):
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0053716
Au Canada, les parents font pression sur leur gouvernement pour avoir un loi: (La CAQ propose l’instauration d’un projet pilote afin de permettre aux parents et enfants malades qui le désirent d’avoir accès à des chambres pressurisées individuelles. Cette mesure est évaluée à 2 millions de dollars. Les parents d’enfants atteints de paralysie cérébrale qui ont essayé les chambres pressurisées savent comment ce traitement peut aider leur enfant à apprendre à parler, à marcher et à développer leurs aptitudes cognitives. Les coûts de location de ces salles étant très dispendieux, ce projet pilote offrira un grand soulagement pour les parents et les enfants qui accepteront d’en bénéficier.) :
https://www.facebook.com/groups/333972306943984/permalink/605140506493828/
En faite première choise que doit être faite en france : c’est de permettre et solisiter les caissons hyperbare déjà Existent de metre en place les tests cliniques pediatques pour maladies neurologiques suivant :
-AVC
-anoxie cérébrale:
http://brain-injury-hope.com/2018/08/kristal-carlson-testimonials/ ( après anglais vous avez traduction en français)
-autisme
Et paralysie cérébrale
(Sur ses 4 problèmes neurologiques il y a déjà des tests cliniques et publications des résultats prometteurs dans autres pays pourquoi pas en france?)
Surtout que : Hbot présente très peu de risques de complications majeures, particulièrement à des pressions inférieures à 1,75 ATA (on a besoins que des petits pressions pour conditions neurologiques.)
En fait, les risques de Hbot sont minimes lorsque les techniciens obéissent aux règles de sécurité et suivent un protocole spécifique. Il n’en résulte que de rares accidents de décompression.
Le centre hyperbare le plus connu en France pour indications neurologiques mais pour adultes est à Nice. (Dr Bernard Gamain ) médecin hyperbare au CHU de NICE . Pourquoi pas des recherches pour les enfants pour les problèmes neurologiques???
MES ACTIONS MISES EN PLACE:
Création de page Facebook personnelle avec expérience et progrès de Mon enfant (arrêt cardiaque et anoxie cérébrale) après utilisation thérapie de caisson hyperbare en Israël : avec un seul but : informer les autres parents :
https://www.facebook.com/groups/333972306943984/
J’ai aussi mit au courant et envoyer les vidéos (avant / et après thérapie caisson hyperbare de Mon fils ) et le compte rendu d’israël a responsable de Hbot à Lyon
Dr Thierry Joffre – Responsable médical du
Centre de Médecine Hyperbare
Tél. 04 72 11 00 31
thierry.joffre@chu-lyon.fr
Voici son impression de progrès de Mon fils apres Hbot : « Vous avez un petit garçon très mignon avec un super sourire : j’ai parcouru l’ensemble des vidéos et effectivement les progrès sont très importants surtout au niveau de son bras gauche : les vidéos de juin montre une « négligence » de la main gauche qui ne sert principalement que d’appui avec un manque de flexion du poignet. Les séquences de septembre et d’octobre sont complètement différentes avec une préhension fine des objets par la main gauche et une flexion du poignet (video du vélo dans le centre commercial).
Au niveau du membre inférieur , le steppage (=boiterie) de la jambe gauche bien visible sur la vidéo de juillet a bien diminué et la vidéo de septembre (montée d’escalier) ne montre quasiment plus rien.
Juste une question (à poser au kiné de TelAvis) : ne pourrait-on pas remplacer l’orthèse (attelle) de cheville gauche par une paire de chaussure montant type basket ? Sur certaines vidéos , Marc ne la met pas et cela n’a pas l’air de poser trop de problèmes à la marche (avec peut être un risque accru de foulure de cheville).
On ne peut espérer que sur les prochaines vidéos on l’entendra parler un peu plus .
En tout cas , Marc a bien progressé et possède certainement beaucoup courage et de patience (peu de caprices sur les vidéos) .. Super ! »
LES SOLUTIONS
Permettre les caissons hyperbares déjà existants en france être accessible au patients et parents qui suette essayer cet thérapie pour leur enfant (sans être oubliger partir à l’étranger !) et adapter la thérapie pour conditions neurologiques semons les études déjà existante !
En France, c’est complètement inaccessible sans la prescription du médecin traitant et du fait que ce ne soit pas reconnu pour des cas comme celui de mon fils, il est impossible de l’obtenir, même en payant, à des coûts au moins abordables pour les parents….c’est scandaleux….
J’ai pu ca meme avoir la réponse de Medecin Hbot à Lyon en france mais meme si on arrive avoir la prescription de son Neuropediatre ou Pediatre (miracle en france!)…. pour Hbot ….problème que on a pas de protocole reconnu et pas beaucoup d’expérience en france pour les enfants sur l’hbot et les indications neurologiques……En france protocole de Hbot ne convienne pas du tout pour les enfants :
(Ca peut être toxique meme)
Pour les enfants on doit utiliser seulement :
60 min
Et 1,5ata
100% oxigen
Meme pour les adultes à Israel ils utilise que 2ata
120min
Et 100% oxigen
Donc ca peut faire plus de mal que de bien utiliser 2,5 ata pour les cas neurologiques en plus si gros pression augmente les risques des effets secondaires….
Malheureusement en France centres Hbot ne réalisent pas des tables 1.5 ou 2 ATA. La table 2.5 ATA est la plus utilisée en France et il n’y a que la durée qui peut différer entre les centre (De 90 à 120 minutes pour les pathologies chroniques.
le CMH de Nice possède une plus grosse expérience sur Hbot et les indications neurologiques (principalement chez l’adulte) en France.
DOCUMENTS COMPLEMENTAIRES
Articles:
Article 1: Paralysie cérébrale :
Lisez mes présidents articles sur hbot!
Et celle-ci :
http://www.therapiehyperbare.com/images/hyperbare/2007-12_oth_pc_marois_aaps.pdf
Article2: AVC (résultats publiés de test clinique officiellement reconnu)en anglais :
https://www.ncbi.nlm.nih.gov/m/pubmed/23335971/
Article 3: accident traumatisme crânien :(résultats publiés de test clinique officiellement reconnu) en anglais :
https://www.ncbi.nlm.nih.gov/m/pubmed/24260334/
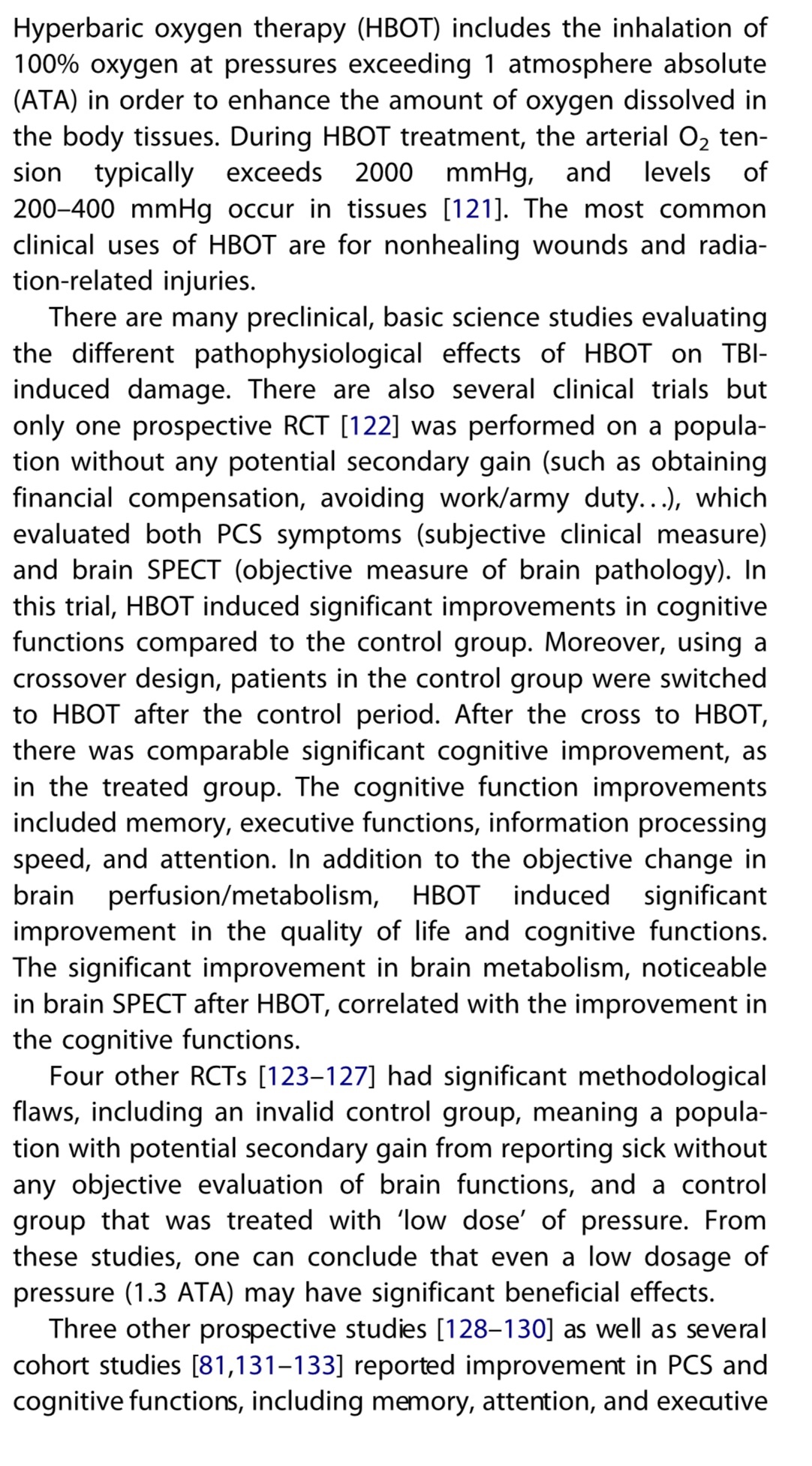
Article 4: réflections sur Hbot et son utilité pour les maladies neurologiques :(anglais)
http://www.tandfonline.com/doi/full/10.1586/14737175.2014.884928
Article 5 de 2014 en français :
http://m.ledevoir.com/article-405133
Article 6: (publication étude d’israël 2013)
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0053716
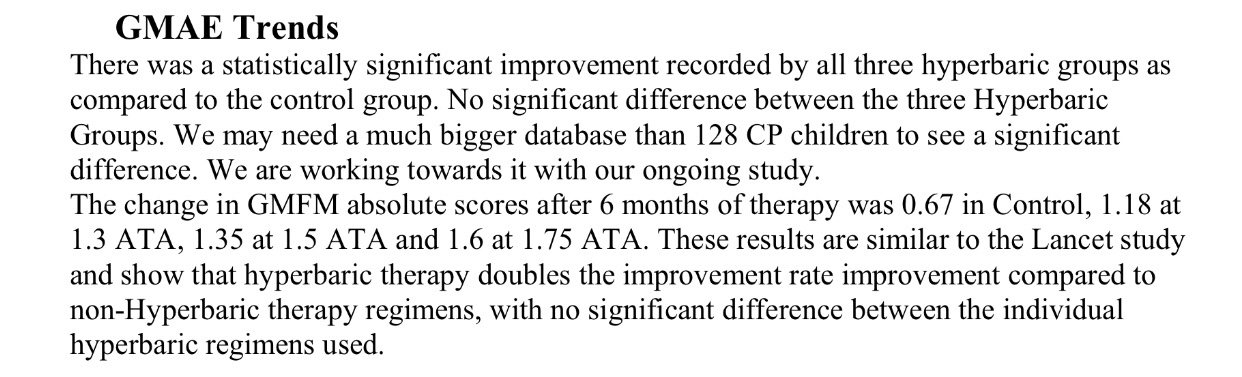
Et PS: que tous les articles /études scientifiques est fait que pour les chambres hyperbare « dur » en metal utiliser en hôpitaux et sellons protocole surveillée. (En aucune cas ça ne peut pas prouver efficacité pour les cambres hyperbares souples pour lesquelles on a que des témoignages des parents). Et une étude lire cet article : http://brain-injury-hope.com/2018/08/study-which-compares-different-pressures-for-cp-in-hbot/
Article de Canada (en images)